Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
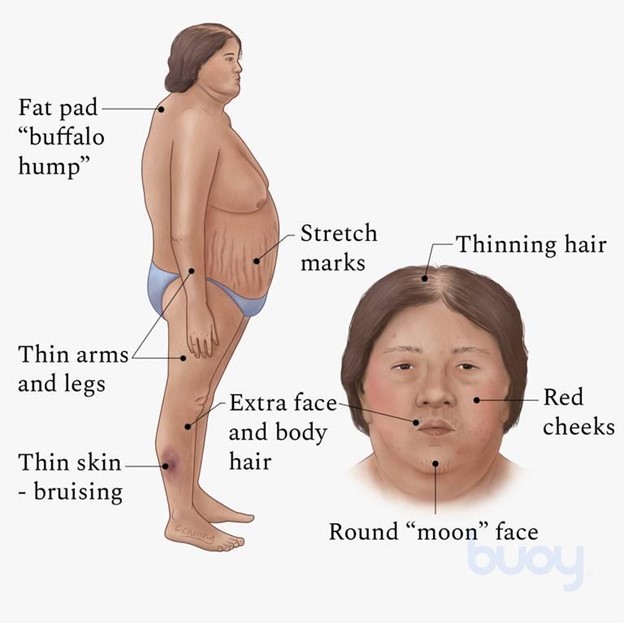
A client admitted to a medical-surgical unit for surgery has a history of Cushing's syndrome. Which physical assessment finding would the nurse expect to observe?
A. Buffalo hump and moon face
Reason: Buffalo hump and moon face are physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, as they indicate fat redistribution and accumulation due to excess cortisol production.
B. Dry, scaly skin and cold intolerance
Reason: Dry, scaly skin and cold intolerance are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hypothyroidism, which affects the metabolism and skin condition.
C. Dry, sticky mucous membranes and hypovolemia
Reason: Dry, sticky mucous membranes and hypovolemia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate dehydration or diabetes insipidus, which affect the fluid balance and urine output.
D. Exophthalmos and tachycardia
Reason: Exophthalmos and tachycardia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hyperthyroidism, which affects the eye protrusion and heart rate.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 3. Take the full exam now
Full Explanation
Choice A Reason: Buffalo hump and moon face are physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, as they indicate fat redistribution and accumulation due to excess cortisol production.
Choice B Reason: Dry, scaly skin and cold intolerance are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hypothyroidism, which affects the metabolism and skin condition.
Choice C Reason: Dry, sticky mucous membranes and hypovolemia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate dehydration or diabetes insipidus, which affect the fluid balance and urine output.
Choice D Reason: Exophthalmos and tachycardia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hyperthyroidism, which affects the eye protrusion and heart rate.
Similar Questions
A nurse enters the room of a client with type 1 diabetes mellitus and finds the client difficult to arouse. The client's skin is warm and flushed and the pulse and respiratory rate are increased from the client's baseline. The nurse would first take which action?
A. Assist the RN to prepare an intravenous (IV) insulin infusion.
Reason: Assisting the RN to prepare an IV insulin infusion is not the first action that the nurse should take, as it may not be appropriate for the client's condition without knowing the blood glucose level.
B. Give the client 4 oz of orange juice.
Reason: Giving the client 4 oz of orange juice is not the first action that the nurse should take, as it may worsen the client's condition if the blood glucose level is high.
C. Check the client's capillary blood glucose.
Reason: Checking the client's capillary blood glucose is the first action that the nurse should take, as it helps to determine if the client has hyperglycemia or hypoglycemia and guides the appropriate intervention.
D. Assist the RN to administer 50% dextrose.
Reason: Assisting the RN to administer 50% dextrose is not the first action that the nurse should take, as it may be harmful for the client if the blood glucose level is high.
Full Explanation
Choice A Reason: Assisting the RN to prepare an IV insulin infusion is not the first action that the nurse should take, as it may not be appropriate for the client's condition without knowing the blood glucose level.
Choice B Reason: Giving the client 4 oz of orange juice is not the first action that the nurse should take, as it may worsen the client's condition if the blood glucose level is high.
Choice C Reason: Checking the client's capillary blood glucose is the first action that the nurse should take, as it helps to determine if the client has hyperglycemia or hypoglycemia and guides the appropriate intervention.
Choice D Reason: Assisting the RN to administer 50% dextrose is not the first action that the nurse should take, as it may be harmful for the client if the blood glucose level is high.
A nurse is collecting data from a client who has diabetes mellitus. The client is confused, flushed, and has an acetone odor on his breath. The nurse should anticipate a prescription for which of the following types of insulin to treat the client?
A. Lantus
Reason: Lantus is not a type of insulin that can treat this client, as it is a long-acting insulin that has no peak effect and lasts for 24 hours.
B. NPH
Reason: NPH is not a type of insulin that can treat this client, as it is an intermediate-acting insulin that peaks in 6 to 8 hours and lasts for 12 to 18 hours.
C. Regular
Reason: Regular is a type of insulin that can treat this client, as it is a short-acting insulin that peaks in 2 to 4 hours and lasts for 6 to 8 hours. It can be used to correct high blood glucose levels and treat diabetic ketoacidosis (DKA), which is indicated by confusion, flushing, and acetone breath.
D. Lispro
Reason: Lispro is not a type of insulin that can treat this client, as it is a rapid-acting insulin that peaks in 30 minutes and lasts for 3 to 5 hours. It can be used to cover meals or snacks but not to treat DKA.
Full Explanation
Choice A Reason: Lantus is not a type of insulin that can treat this client, as it is a long-acting insulin that has no peak effect and lasts for 24 hours.
Choice B Reason: NPH is not a type of insulin that can treat this client, as it is an intermediate-acting insulin that peaks in 6 to 8 hours and lasts for 12 to 18 hours.
Choice C Reason: Regular is a type of insulin that can treat this client, as it is a short-acting insulin that peaks in 2 to 4 hours and lasts for 6 to 8 hours. It can be used to correct high blood glucose levels and treat diabetic ketoacidosis (DKA), which is indicated by confusion, flushing, and acetone breath.
Choice D Reason: Lispro is not a type of insulin that can treat this client, as it is a rapid-acting insulin that peaks in 30 minutes and lasts for 3 to 5 hours. It can be used to cover meals or snacks but not to treat DKA.
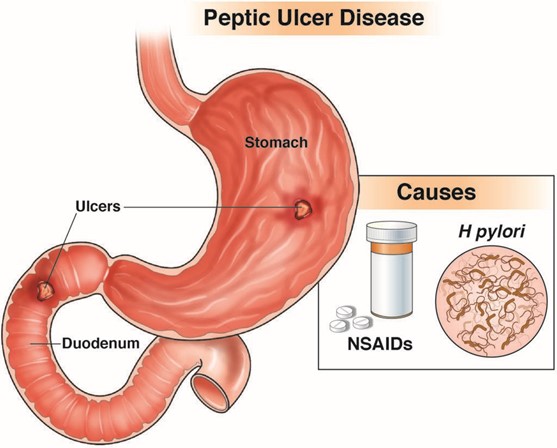
A client was admitted in the hospital with peptic ulcer disease tells the nurse about having black tarry stools. Which of the following is the most appropriate nursing action?
A. Instruct the client to increase fluid intake.
Reason: Instructing the client to increase fluid intake is not the most appropriate nursing action, as it does not address the cause or severity of the bleeding.
B. Notify the health care provider.
Reason: Notifying the health care provider is the most appropriate nursing action, as it indicates that the client may have a bleeding ulcer that requires immediate evaluation and treatment.
C. Advise the client to take iron rich foods.
Reason: Advising the client to take iron rich foods is not the most appropriate nursing action, as it does not prevent or correct anemia or bleeding.
D. Document the findings.
Reason: Documenting the findings is not the most appropriate nursing action, as it does not initiate any intervention or outcome.
Full Explanation
Choice A Reason: Instructing the client to increase fluid intake is not the most appropriate nursing action, as it does not address the cause or severity of the bleeding.
Choice B Reason: Notifying the health care provider is the most appropriate nursing action, as it indicates that the client may have a bleeding ulcer that requires immediate evaluation and treatment.
Choice C Reason: Advising the client to take iron rich foods is not the most appropriate nursing action, as it does not prevent or correct anemia or bleeding.
Choice D Reason: Documenting the findings is not the most appropriate nursing action, as it does not initiate any intervention or outcome.