Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A client has a patch test performed with the following results. Which of the following is the best response the nurse will offer the client regarding the observations from the test?
A. The test assesses for sun protection factor
Reason: The test does not assess for sun protection factor, but rather for contact dermatitis. Sun protection factor is a measure of how well a sunscreen protects the skin from ultraviolet radiation, which can cause sunburn and skin damage.
B. The test is inconclusive
Reason: The test is not inconclusive, but rather positive for some allergens and negative for others. The test involves applying small patches of different substances to the skin and observing for any reactions after 48 hours.
C. The presence of erythema indicates you are allergic to the allergen
Reason: This is the correct choice. The presence of erythema indicates you are allergic to the allergen, as it shows inflammation and irritation of the skin due to an immune response. Erythema is redness of the skin that can be accompanied by itching, swelling, or blisters.
D. The areas that did not turn red indicate low risk for skin cancer
Reason: The areas that did not turn red do not indicate low risk for skin cancer, but rather no reaction to the allergen. Skin cancer is a malignant growth of abnormal cells in the skin that can be caused by various factors, such as genetic mutations, exposure to carcinogens, or immunosuppression.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: The test does not assess for sun protection factor, but rather for contact dermatitis. Sun protection factor is a measure of how well a sunscreen protects the skin from ultraviolet radiation, which can cause sunburn and skin damage.
Choice B Reason: The test is not inconclusive, but rather positive for some allergens and negative for others. The test involves applying small patches of different substances to the skin and observing for any reactions after 48 hours.
Choice C Reason: This is the correct choice. The presence of erythema indicates you are allergic to the allergen, as it shows inflammation and irritation of the skin due to an immune response. Erythema is redness of the skin that can be accompanied by itching, swelling, or blisters.
Choice D Reason: The areas that did not turn red do not indicate low risk for skin cancer, but rather no reaction to the allergen. Skin cancer is a malignant growth of abnormal cells in the skin that can be caused by various factors, such as genetic mutations, exposure to carcinogens, or immunosuppression.
Similar Questions
A nurse is assessing a client who is receiving total parenteral nutrition (TPN) therapy via an infusion pump. Which of the following actions should the nurse take?
A. Obtain the client's blood glucose every 12 hr.
Reason: Obtaining the client's blood glucose every 12 hr is not enough, as the nurse should monitor it more frequently, at least every 4 to 6 hr, to prevent hyperglycemia or hypoglycemia. TPN is a high-glucose solution that can affect the blood sugar levels.
B. Change the IV site dressing every 4 days.
Reason: Changing the IV site dressing every 4 days is not enough, as the nurse should change it daily or as needed to prevent infection. TPN is a high-risk solution that can introduce microorganisms into the bloodstream.
C. Change the IV tubing every 24 hr.
Reason: This is the correct choice. Changing the IV tubing every 24 hr is recommended to prevent infection and maintain sterility. TPN is a complex solution that can support bacterial growth and contamination.
D. Weigh the client every other day.
Reason: Weighing the client every other day is not enough, as the nurse should weigh the client daily to evaluate fluid balance and nutritional status. TPN can cause fluid retention or depletion, as well as weight gain or loss.
Full Explanation
Choice A Reason: Obtaining the client's blood glucose every 12 hr is not enough, as the nurse should monitor it more frequently, at least every 4 to 6 hr, to prevent hyperglycemia or hypoglycemia. TPN is a high-glucose solution that can affect the blood sugar levels.
Choice B Reason: Changing the IV site dressing every 4 days is not enough, as the nurse should change it daily or as needed to prevent infection. TPN is a high-risk solution that can introduce microorganisms into the bloodstream.
Choice C Reason: This is the correct choice. Changing the IV tubing every 24 hr is recommended to prevent infection and maintain sterility. TPN is a complex solution that can support bacterial growth and contamination.
Choice D Reason: Weighing the client every other day is not enough, as the nurse should weigh the client daily to evaluate fluid balance and nutritional status. TPN can cause fluid retention or depletion, as well as weight gain or loss.
A client arrives to the emergency department after falling from a ladder. The client has a loss of sensation and flaccid paralysis. Which of the following complications of an acute spinal cord injury does the nurse suspect?
A. Hemorrhage
Reason: Hemorrhage is not a complication of an acute spinal cord injury, but rather a possible cause of it. Hemorrhage can occur due to trauma or rupture of blood vessels in or around the spinal cord, leading to compression and damage of the nerve tissue.
B. Spinal shock
Reason: This is the correct choice. Spinal shock is a complication of an acute spinal cord injury that occurs within minutes to hours after the injury. It is characterized by loss of sensation, motor function, reflexes, and autonomic function below the level of injury. It is caused by transient disruption of nerve conduction and synaptic transmission in the spinal cord.
C. Apoptosis
Reason: Apoptosis is not a complication of an acute spinal cord injury, but rather a cellular process that occurs after it. Apoptosis is programmed cell death that occurs in response to injury or stress. It can lead to further loss of neurons and glial cells in the spinal cord over time.
D. Neurogenic shock
Reason: Neurogenic shock is a complication of an acute spinal cord injury that occurs within hours to days after the injury. It is characterized by hypotension, bradycardia, and peripheral vasodilation due to loss of sympathetic tone and unopposed parasympathetic activity. It is caused by disruption of autonomic pathways in the spinal cord.
Full Explanation
Choice A Reason: Hemorrhage is not a complication of an acute spinal cord injury, but rather a possible cause of it. Hemorrhage can occur due to trauma or rupture of blood vessels in or around the spinal cord, leading to compression and damage of the nerve tissue.
Choice B Reason: This is the correct choice. Spinal shock is a complication of an acute spinal cord injury that occurs within minutes to hours after the injury. It is characterized by loss of sensation, motor function, reflexes, and autonomic function below the level of injury. It is caused by transient disruption of nerve conduction and synaptic transmission in the spinal cord.
Choice C Reason: Apoptosis is not a complication of an acute spinal cord injury, but rather a cellular process that occurs after it. Apoptosis is programmed cell death that occurs in response to injury or stress. It can lead to further loss of neurons and glial cells in the spinal cord over time.
Choice D Reason: Neurogenic shock is a complication of an acute spinal cord injury that occurs within hours to days after the injury. It is characterized by hypotension, bradycardia, and peripheral vasodilation due to loss of sympathetic tone and unopposed parasympathetic activity. It is caused by disruption of autonomic pathways in the spinal cord.
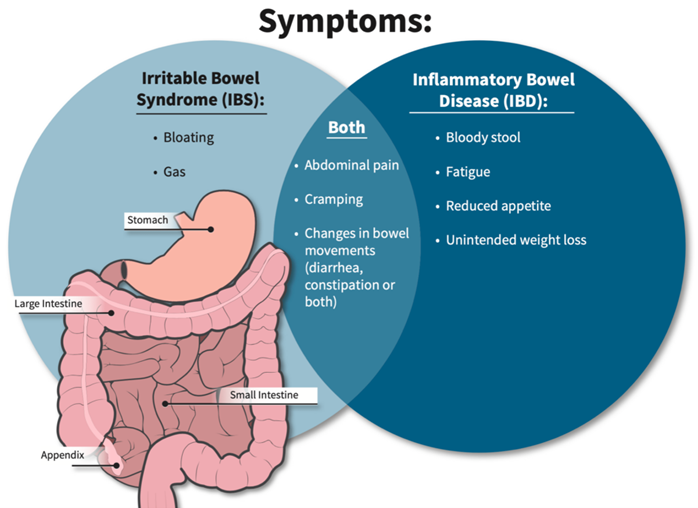
A nurse provides education to a client diagnosed with inflammatory bowel syndrome (IBS) about measures to treat diarrhea caused by acute flare-ups. Which statement by the client indicates a need for further teaching?
A. "I will eat frequent small meals."
reason: This is correct because eating frequent small meals can help the client with IBS to avoid overloading the digestive system and triggering diarrhea. The nurse should advise the client to eat slowly and chew well, and avoid foods that are spicy, fatty, or gas-producing.
B. "I will increase the intake of leafy greens and other sources of dietary fiber."
reason: This is incorrect because increasing the intake of leafy greens and other sources of dietary fiber can worsen diarrhea by increasing stool bulk and motility. The nurse should advise the client to limit or avoid high-fiber foods, such as whole grains, fruits, vegetables, nuts, and seeds, during acute flare-ups of IBS. The client can gradually reintroduce fiber when the symptoms subside.
C. "I will increase fluids."
reason: This is correct because increasing fluids can help the client with IBS to prevent dehydration and electrolyte imbalance caused by diarrhea. The nurse should advise the client to drink at least 8 glasses of water per day and avoid caffeinated, alcoholic, or carbonated beverages that can irritate the bowel or cause gas.
D. "I will take prescribed medications on schedule to regulate bowel patterns."
reason: This is correct because taking prescribed medications on schedule can help the client with IBS to regulate bowel patterns and reduce diarrhea. The nurse should instruct the client on how to use medications, such as antidiarrheals, antispasmodics, or probiotics, as ordered by the provider. The nurse should also monitor the client for any adverse effects or interactions of the medications.
Full Explanation
Choice A reason: This is correct because eating frequent small meals can help the client with IBS to avoid overloading the digestive system and triggering diarrhea. The nurse should advise the client to eat slowly chew well, and avoid foods that are spicy, fatty, or gas-producing.
Choice B reason: This is incorrect because increasing the intake of leafy greens and other sources of dietary fiber can worsen diarrhea by increasing stool bulk and motility. The nurse should advise the client to limit or avoid high-fiber foods, such as whole grains, fruits, vegetables, nuts, and seeds, during acute flare-ups of IBS. The client can gradually reintroduce fiber when the symptoms subside.
Choice C reason: This is correct because increasing fluids can help the client with IBS to prevent dehydration and electrolyte imbalance caused by diarrhea. The nurse should advise the client to drink at least 8 glasses of water per day and avoid caffeinated, alcoholic, or carbonated beverages that can irritate the bowel or cause gas.
Choice D reason: This is correct because taking prescribed medications on schedule can help the client with IBS to regulate bowel patterns and reduce diarrhea. The nurse should instruct the client on how to use medications, such as antidiarrheals, antispasmodics, or probiotics, as ordered by the provider. The nurse should also monitor the client for any adverse effects or interactions of the medications.