Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A client has been brought to the emergency department with abdominal pain and is subsequently diagnosed with appendicitis. The client is scheduled for an appendectomy but questions the nurse about how his health will be affected by the absence of an appendix. How should the nurse best respond?
A. The surgeon will encourage you to limit your fat intake for a few weeks after the surgery, but your body will then begin to compensate.
This statement is not the best response for the nurse to give. The surgeon will not encourage the client to limit their fat intake after an appendectomy, as this has nothing to do with the appendix. The appendix is a small pouch attached to the beginning of the large intestine, not the small intestine where most of the fat digestion and absorption occurs.
B. Your appendix doesn't play a major role so you won't notice any difference after your recovery from surgery.
This statement is not the best response for the nurse to give. The appendix does play a role in the immune system and the gut microbiome, as it contains lymphoid tissue and beneficial bacteria. The client may notice some changes in their immunity or digestion after an appendectomy, especially if they have an infection or take antibiotics.
C. Your body will absorb slightly fewer nutrients from the food you eat, but you won't be aware of this.
This statement is not the best response for the nurse to give. The appendix does not affect the absorption of nutrients from the food the client eats, as it is not involved in the digestive process. The appendix is located at the end of the small intestine, where most of the nutrients have already been absorbed.
D. Your small intestine will adapt over time to the absence of your appendix.
This statement is the best response for the nurse to give. The appendix is not essential for survival, and the small intestine can adapt to its removal over time. The client may experience some temporary symptoms such as diarrhea, bloating, or gas after an appendectomy, but these usually resolve within a few weeks. The nurse should reassure the client that they can live a normal and healthy life without an appendix.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Med Surg Nursing 102 Proctored Exam 4. Take the full exam now
Full Explanation
Choice A reason: This statement is not the best response for the nurse to give. The surgeon will not encourage the client to limit their fat intake after an appendectomy, as this has nothing to do with the appendix. The appendix is a small pouch attached to the beginning of the large intestine, not the small intestine where most of the fat digestion and absorption occurs.
Choice B reason: This statement is not the best response for the nurse to give. The appendix does play a role in the immune system and the gut microbiome, as it contains lymphoid tissue and beneficial bacteria. The client may notice some changes in their immunity or digestion after an appendectomy, especially if they have an infection or take antibiotics.
Choice C reason: This statement is not the best response for the nurse to give. The appendix does not affect the absorption of nutrients from the food the client eats, as it is not involved in the digestive process. The appendix is located at the end of the small intestine, where most of the nutrients have already been absorbed.
Choice D reason: This statement is the best response for the nurse to give. The appendix is not essential for survival, and the small intestine can adapt to its removal over time. The client may experience some temporary symptoms such as diarrhea, bloating, or gas after an appendectomy, but these usually resolve within a few weeks. The nurse should reassure the client that they can live a normal and healthy life without an appendix.
Similar Questions
A nurse is assessing four clients for fluid balance. The nurse should identify that which of the following manifestations of dehydration?
A. A client who has a urine specific gravity of 1.010. (Reference Range 1.005-1.030)
A client who has a urine specific gravity of 1.010 is not dehydrated. Urine specific gravity is a measure of the concentration of solutes in the urine. A normal range is 1.005-1.030, which means that the urine is neither too dilute nor too concentrated. A high urine specific gravity (>1.030) indicates dehydration, as the urine becomes more concentrated due to fluid loss. A low urine specific gravity (<1.005) indicates overhydration, as the urine becomes more dilute due to fluid excess.
B. A client who has a hematocrit of 42%. (Reference Range 36-46%)
A client who has a hematocrit of 42% is not dehydrated. Hematocrit is the percentage of red blood cells in the blood. A normal range is 36-46% for women and 40-54% for men. A high hematocrit (>54% for men and >46% for women) indicates dehydration, as the blood becomes more viscous due to fluid loss. A low hematocrit (<40% for men and <36% for women) indicates overhydration, as the blood becomes more diluted due to fluid excess.
C. A client who has a temperature of 39 °C.
A client who has a temperature of 39 °C may or may not be dehydrated. Temperature is a measure of the body's heat production and regulation. A normal range is 36.5-37.5 °C. A high temperature (>37.5 °C) indicates fever, which can be caused by various factors, such as infection, inflammation, or medication. Fever can also cause dehydration, as the body loses fluid through sweating and increased respiration. However, fever is not a specific sign of dehydration, as there may be other causes or contributing factors.
D. A client who has a weight loss of 2.2 kg in 24 hr.
A client who has a weight loss of 2.2 kg in 24 hr is dehydrated. Weight loss is a measure of the change in the body's mass over time. A normal range is 0.5-1 kg per week. A rapid weight loss (>1 kg per day) indicates dehydration, as the body loses fluid through various routes, such as urine, stool, sweat, or vomit. Weight loss is a sensitive and reliable sign of dehydration, as it reflects the amount of fluid loss.
Full Explanation
Choice A reason: A client who has a urine specific gravity of 1.010 is not dehydrated. Urine specific gravity is a measure of the concentration of solutes in the urine. A normal range is 1.005-1.030, which means that the urine is neither too dilute nor too concentrated. A high urine specific gravity (>1.030) indicates dehydration, as the urine becomes more concentrated due to fluid loss. A low urine specific gravity (<1.005) indicates overhydration, as the urine becomes more dilute due to fluid excess.
Choice B reason: A client who has a hematocrit of 42% is not dehydrated. Hematocrit is the percentage of red blood cells in the blood. A normal range is 36-46% for women and 40-54% for men. A high hematocrit (>54% for men and >46% for women) indicates dehydration, as the blood becomes more viscous due to fluid loss. A low hematocrit (<40% for men and <36% for women) indicates overhydration, as the blood becomes more diluted due to fluid excess.
Choice C reason: A client who has a temperature of 39 °C may or may not be dehydrated. Temperature is a measure of the body's heat production and regulation. A normal range is 36.5-37.5 °C. A high temperature (>37.5 °C) indicates fever, which can be caused by various factors, such as infection, inflammation, or medication. Fever can also cause dehydration, as the body loses fluid through sweating and increased respiration. However, fever is not a specific sign of dehydration, as there may be other causes or contributing factors.
Choice D reason: A client who has a weight loss of 2.2 kg in 24 hr is dehydrated. Weight loss is a measure of the change in the body's mass over time. A normal range is 0.5-1 kg per week. A rapid weight loss (>1 kg per day) indicates dehydration, as the body loses fluid through various routes, such as urine, stool, sweat, or vomit. Weight loss is a sensitive and reliable sign of dehydration, as it reflects the amount of fluid loss.
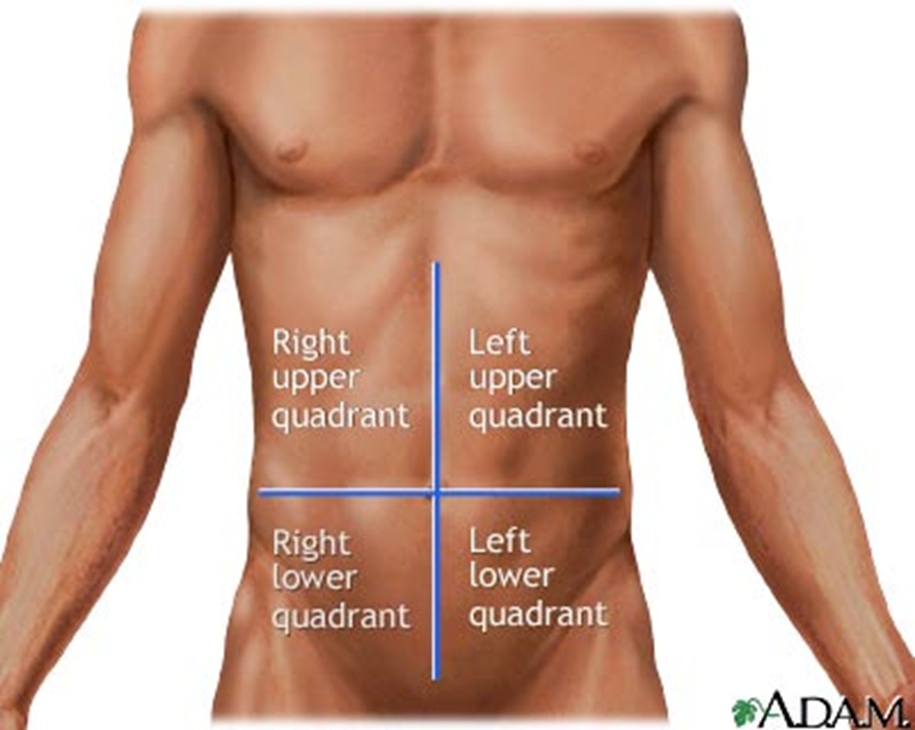
A nurse is admitting a client with suspected appendicitis. Identify where the nurse will palpate to assess for pain at McBurney's point. (Selectable areas, or "Hot Spots," are outlined in the artwork below. Select only the outlined area that corresponds to your answer)
A. Upper right quadrant
The upper right quadrant is not the correct location for McBurney's point. This quadrant contains the liver, gallbladder, right kidney, and part of the colon. Pain in this area may indicate problems with these organs, such as hepatitis, gallstones, or kidney infection.
B. Upper left quadrant
The upper left quadrant is not the correct location for McBurney's point. This quadrant contains the stomach, spleen, left kidney, and part of the colon. Pain in this area may indicate problems with these organs, such as gastritis, splenomegaly, or kidney stones.
C. Lower right quadrant
The lower right quadrant is the correct location for McBurney's point. This quadrant contains the appendix, right ovary, and right fallopian tube. McBurney's point is a point on the abdomen that is one-third of the distance from the right anterior superior iliac spine to the umbilicus. Pain in this area may indicate appendicitis, ovarian cyst, or ectopic pregnancy.
D. Lower left quadrant
The lower left quadrant is not the correct location for McBurney's point. This quadrant contains the sigmoid colon, left ovary, and left fallopian tube. Pain in this area may indicate problems with these organs, such as diverticulitis, ovarian torsion, or pelvic inflammatory disease.
Full Explanation
Choice A reason: The upper right quadrant is not the correct location for McBurney's point. This quadrant contains the liver, gallbladder, right kidney, and part of the colon. Pain in this area may indicate problems with these organs, such as hepatitis, gallstones, or kidney infection.
Choice B reason: The upper left quadrant is not the correct location for McBurney's point. This quadrant contains the stomach, spleen, left kidney, and part of the colon. Pain in this area may indicate problems with these organs, such as gastritis, splenomegaly, or kidney stones.
Choice C reason: The lower right quadrant is the correct location for McBurney's point. This quadrant contains the appendix, right ovary, and right fallopian tube. McBurney's point is a point on the abdomen that is one-third of the distance from the right anterior superior iliac spine to the umbilicus. Pain in this area may indicate appendicitis, ovarian cyst, or ectopic pregnancy.
Choice D reason: The lower left quadrant is not the correct location for McBurney's point. This quadrant contains the sigmoid colon, left ovary, and left fallopian tube. Pain in this area may indicate problems with these organs, such as diverticulitis, ovarian torsion, or pelvic inflammatory disease.
A nurse is discussing safety for administering intravenous fluids. Which condition might occur if hypertonic solutions are administered too quickly?
A. Mental alertness
Mental alertness is not affected by the administration of hypertonic solutions. Hypertonic solutions are fluids that have a higher concentration of solutes than the blood. They draw water out of the cells and into the blood vessels, increasing the blood volume and osmolarity.
B. Decreased pulse
Decreased pulse is not a result of administering hypertonic solutions too quickly. On the contrary, hypertonic solutions can increase the pulse rate as they increase the blood volume and pressure.
C. Decreased blood pressure
Decreased blood pressure is not a consequence of administering hypertonic solutions too quickly. Hypertonic solutions can raise the blood pressure as they increase the blood volume and osmolarity.
D. Fluid overload
Fluid overload is the correct answer. Administering hypertonic solutions too quickly can cause fluid overload, which is a condition where the body has too much fluid in the blood vessels. This can lead to symptoms such as edema, dyspnea, crackles, and weight gain. Fluid overload can also cause heart failure, pulmonary edema, and cerebral edema.
Full Explanation
Choice A reason: Mental alertness is not affected by the administration of hypertonic solutions. Hypertonic solutions are fluids that have a higher concentration of solutes than the blood. They draw water out of the cells and into the blood vessels, increasing the blood volume and osmolarity.
Choice B reason: Decreased pulse is not a result of administering hypertonic solutions too quickly. On the contrary, hypertonic solutions can increase the pulse rate as they increase the blood volume and pressure.
Choice C reason: Decreased blood pressure is not a consequence of administering hypertonic solutions too quickly. Hypertonic solutions can raise the blood pressure as they increase the blood volume and osmolarity.
Choice D reason: Fluid overload is the correct answer. Administering hypertonic solutions too quickly can cause fluid overload, which is a condition where the body has too much fluid in the blood vessels. This can lead to symptoms such as edema, dyspnea, crackles, and weight gain. Fluid overload can also cause heart failure, pulmonary edema, and cerebral edema.