Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A client whose hyperthyroidism has not been responsive to medications is admitted for evaluation. During the admission assessment the client reports to the nurse of a sudden onset of feeling apprehensive and nurse notes the client is restless and very warm to touch. Which action should the nurse implement next?
A. Access laboratory results to confirm a thyroid crisis.
Accessing laboratory results to confirm a thyroid crisis is important, but the clinical presentation of the client with sudden onset symptoms and a known history of uncontrolled hyperthyroidism suggests the need for immediate intervention rather than waiting for laboratory confirmation.
B. Obtain a complete set of vital signs.
Obtaining a complete set of vital signs is an important assessment to gather comprehensive data, but in the case of a suspected thyroid crisis, immediate intervention takes precedence over obtaining vital signs.
C. Initiate intravenous access.
In this scenario, the client's sudden onset of feeling apprehensive, restlessness, and increased body temperature are consistent with symptoms of a thyroid crisis, also known as thyroid storm or thyrotoxic crisis. Thyroid crisis is a life-threatening condition that requires immediate medical intervention. Initiating IV access is crucial to ensure the prompt administration of medications and fluids to manage the thyroid crisis effectively. IV access allows for the administration of beta-blockers, antithyroid drugs, and supportive care, which are essential components of the treatment for thyroid crisis. IV access also provides a route for fluid resuscitation if necessary.
D. Encourage relaxation and slow deep breathing.
Encouraging relaxation and slow deep breathing may be beneficial in managing anxiety or discomfort, but it does not address the underlying emergency situation of a thyroid crisis. The nurse should focus on initiating appropriate medical interventions first.
This question is an excerpt from Nurse Dive's nursing test bank - RN Hesi Exit Proctored Exam. Take the full exam now
Full Explanation
In this scenario, the client's sudden onset of feeling apprehensive, restlessness, and increased body temperature are consistent with symptoms of a thyroid crisis, also known as thyroid storm or thyrotoxic crisis. Thyroid crisis is a life-threatening condition that requires immediate medical intervention.
Initiating IV access is crucial to ensure the prompt administration of medications and fluids to manage the thyroid crisis effectively. IV access allows for the administration of beta-blockers, antithyroid drugs, and supportive care, which are essential components of the treatment for thyroid crisis. IV access also provides a route for fluid resuscitation if necessary.
Accessing laboratory results to confirm a thyroid crisis is important, but the clinical presentation of the client with sudden onset symptoms and a known history of uncontrolled hyperthyroidism suggests the need for immediate intervention rather than waiting for laboratory confirmation.
Obtaining a complete set of vital signs is an important assessment to gather comprehensive data, but in the case of a suspected thyroid crisis, immediate intervention takes precedence over obtaining vital signs.
Encouraging relaxation and slow deep breathing may be beneficial in managing anxiety or discomfort, but it does not address the underlying emergency situation of a thyroid crisis. The nurse should focus on initiating appropriate medical interventions first.
Similar Questions
The nurse is setting up the equipment to assist with a sigmoidoscopy while the practical nurse (PN) positions the client in a flat prone position. Which action should the nurse implement?
A. Arrange for unlicensed assistive personnel to assist the PN during the procedure.
Arranging for unlicensed assistive personnel to assist the PN during the procedure does not address the incorrect positioning of the client. The priority is to ensure the client is positioned correctly for the sigmoidoscopy, which is typically on the left side with knees drawn toward the chest.
B. Acknowledge that the PN has positioned the client safely and correctly.
Acknowledging that the PN has positioned the client safely and correctly is not appropriate because the flat prone position is incorrect for a sigmoidoscopy. The correct position is on the left side with knees drawn toward the chest.
C. Assume care of the client and assign the PN to the care of a different client.
Assuming care of the client and assigning the PN to the care of a different client does not address the educational opportunity. It is important to demonstrate the correct positioning to the PN to ensure proper care in future procedures.
D. Demonstrate to the PN how to position the client more effectively for the procedure.
Demonstrating to the PN how to position the client more effectively for the procedure is the correct action. This ensures the client is in the proper position for the sigmoidoscopy and provides an educational opportunity for the PN.
Full Explanation
The correct answer is choice D. Demonstrate to the PN how to position the client more effectively for the procedure.
Choice A rationale:
Arranging for unlicensed assistive personnel to assist the PN during the procedure does not address the incorrect positioning of the client. The priority is to ensure the client is positioned correctly for the sigmoidoscopy, which is typically on the left side with knees drawn toward the chest.
Choice B rationale:
Acknowledging that the PN has positioned the client safely and correctly is not appropriate because the flat prone position is incorrect for a sigmoidoscopy. The correct position is on the left side with knees drawn toward the chest.
Choice C rationale:
Assuming care of the client and assigning the PN to the care of a different client does not address the educational opportunity. It is important to demonstrate the correct positioning to the PN to ensure proper care in future procedures.
Choice D rationale:
Demonstrating to the PN how to position the client more effectively for the procedure is the correct action. This ensures the client is in the proper position for the sigmoidoscopy and provides an educational opportunity for the PN.
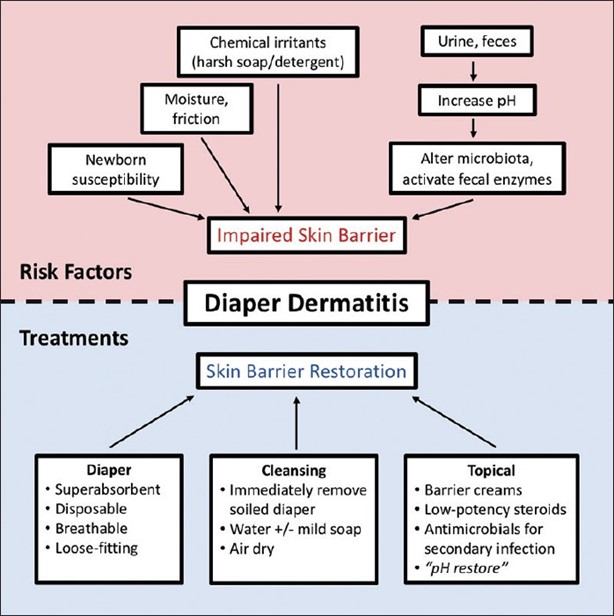
The mother of a 7-month-old brings the infant to the clinic because the skin in the diaper area is excoriated and red, but there are no blisters or bleeding. The mother reports no evidence of watery stools. Which nursing intervention should the nurse implement?
A. Instruct the mother to change the child's diaper more often.
The excoriated and red skin in the diaper area suggests the presence of diaper dermatitis, which is commonly caused by prolonged exposure to moisture and irritants such as urine and feces. Changing the diaper more frequently helps to minimize the exposure to these irritants and promotes better skin hygiene.
B. Ask the mother to decrease the infant's intake of fruits for 24 hours.
Asking the mother to decrease the infant's intake of fruits for 24 hours is not necessary unless there is evidence of diarrhea or specific dietary concerns. Fruits are generally a healthy part of an infant's diet and do not directly cause diaper dermatitis.
C. Encourage the mother to apply lotion with each diaper change.
Encouraging the mother to apply lotion with each diaper change may not be recommended in this case, as lotions and creams can further trap moisture and exacerbate the condition. It is best to keep the area clean and dry.
D. Tell the mother to cleanse with soap and water at each diaper change.
Telling the mother to cleanse with soap and water at each diaper change may be too harsh for the infant's sensitive skin. Plain water or mild, fragrance-free wipes are typically sufficient for cleaning the diaper area. Soap can be drying and irritating to the skin, so it is generally not necessary unless there is a specific indication.
Full Explanation
The excoriated and red skin in the diaper area suggests the presence of diaper dermatitis, which is commonly caused by prolonged exposure to moisture and irritants such as urine and feces. Changing the diaper more frequently helps to minimize the exposure to these irritants and promotes better skin hygiene.
Asking the mother to decrease the infant's intake of fruits for 24 hours is not necessary unless there is evidence of diarrhea or specific dietary concerns. Fruits are generally a healthy part of an infant's diet and do not directly cause diaper dermatitis.
Encouraging the mother to apply lotion with each diaper change may not be recommended in this case, as lotions and creams can further trap moisture and exacerbate the condition. It is best to keep the area clean and dry.
Telling the mother to cleanse with soap and water at each diaper change may be too harsh for the infant's sensitive skin. Plain water or mild, fragrance-free wipes are typically sufficient for cleaning the diaper area. Soap can be drying and irritating to the skin, so it is generally not necessary unless there is a specific indication.
The client is a 7-year-old with spastic cerebral palsy (CP) admitted to pre-op for heel cord lengthening. Child has cognitive and speech delays. Experiences absent seizures numerous times daily according to parent. The nurse is developing the plan of care for the child.
To provide atraumatic care for this child post-operatively, what will be a priority?
A. Pain assessments
Assessing and managing pain is a crucial aspect of providing atraumatic care for any post-operative patient, including a child with spastic cerebral palsy. It is important to monitor and assess the child's pain levels regularly to ensure their comfort and well-being. Pain can be particularly challenging to assess in a child with cognitive and speech delays, so the nurse should use appropriate pain assessment tools and also consider nonverbal cues, changes in behavior, and physiological indicators of pain. While antibiotics may be prescribed if there is an infection present, it is not mentioned as a priority in this specific scenario. The focus is on providing atraumatic care post-operatively. Occupational therapy, physical therapy, and wound care are all important components of the child's overall care, but they may not be the immediate priority post-operatively. The child's specific needs and surgical procedure will determine when these interventions are appropriate and can be incorporated into the plan of care as needed. However, addressing pain is of utmost importance in the immediate post-operative period.
B. Antibiotics
C. Occupational therapy
D. Wound care
E. Physical therapy
Full Explanation
Assessing and managing pain is a crucial aspect of providing atraumatic care for any post-operative patient, including a child with spastic cerebral palsy. It is important to monitor and assess the child's pain levels regularly to ensure their comfort and
well-being. Pain can be particularly challenging to assess in a child with cognitive and speech delays, so the nurse should use appropriate pain assessment tools and also consider nonverbal cues, changes in behavior, and physiological indicators of pain.
While antibiotics may be prescribed if there is an infection present, it is not mentioned as a priority in this specific scenario. The focus is on providing atraumatic care post-operatively.
Occupational therapy, physical therapy, and wound care are all important components of the child's overall care, but they may not be the immediate priority post-operatively. The child's specific needs and surgical procedure will determine when these interventions are appropriate and can be incorporated into the plan of care as needed. However, addressing pain is of utmost importance in the immediate post-operative period.