Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A client with possible acute kidney injury (AKI) is admitted to the hospital and mannitol is prescribed as a fluid challenge. Prior to carrying out this prescription, what intervention should the nurse implement?
A. No specific nursing action is required.
B. Collect a clean catch urine specimen.
Collecting a clean catch urine specimen may be necessary for diagnostic purposes to assess kidney function and determine the presence or severity of acute kidney injury. However, obtaining vital signs and assessing breath sounds should be the first nursing intervention before administering any medication, including mannitol, to ensure the client's safety and monitor for any potential adverse effects.
C. Instruct the client to empty the bladder.
D. Obtain vital signs and breath sounds.
Acute kidney injury (AKI) can have significant impacts on the client's fluid and electrolyte balance. Mannitol, a diuretic, is commonly used to promote diuresis and increase urine output in cases of AKI. However, it is essential to assess the client's hemodynamic status and overall condition before administering mannitol. Obtaining vital signs (such as blood pressure, heart rate, respiratory rate, and temperature) helps evaluate the client's baseline status and monitor for any changes that may occur after administering mannitol. It is particularly important to assess blood pressure as mannitol can potentially cause hypotension as a side effect. Assessing breath sounds is also crucial because pulmonary edema can occur as a complication of AKI. Mannitol administration may exacerbate this condition. Therefore, assessing breath sounds allows the nurse to monitor for signs of fluid overload, such as crackles or wheezes.
This question is an excerpt from Nurse Dive's nursing test bank - RN Hesi Exit Proctored Exam. Take the full exam now
Full Explanation
Acute kidney injury (AKI) can have significant impacts on the client's fluid and electrolyte balance. Mannitol, a diuretic, is commonly used to promote diuresis and increase urine
output in cases of AKI. However, it is essential to assess the client's hemodynamic status and overall condition before administering mannitol.
Obtaining vital signs (such as blood pressure, heart rate, respiratory rate, and temperature) helps evaluate the client's baseline status and monitor for any changes that may occur after administering mannitol. It is particularly important to assess blood pressure as mannitol can potentially cause hypotension as a side effect.
Assessing breath sounds is also crucial because pulmonary edema can occur as a complication of AKI. Mannitol administration may exacerbate this condition. Therefore, assessing breath sounds allows the nurse to monitor for signs of fluid overload, such as crackles or wheezes.
Collecting a clean catch urine specimen may be necessary for diagnostic purposes to assess kidney function and determine the presence or severity of acute kidney injury. However, obtaining vital signs and assessing breath sounds should be the first nursing intervention before administering any medication, including mannitol, to ensure the client's safety and monitor for any potential adverse effects.
Similar Questions
In planning care for a client with early stage Alzheimer's disease, the nurse establishes the nursing problem of risk for injury related to impaired judgment. Which intervention is most important for the nurse to include in this client's plan of care?
A. Engage the client in regularly scheduled activities during the day.
Engaging the client in regularly scheduled activities during the day is a beneficial intervention as it provides structure and stimulation for the client. However, it may not directly address the risk for injury related to impaired judgment.
B. Offer the client frequent reassurance that he/she will be safe.
Offering the client frequent reassurance that they will be safe is important to provide emotional support, but it may not be sufficient in preventing physical harm or addressing the specific nursing problem of risk for injury.
C. Arrange the client's environment so the client can move about freely.
Clients with early-stage Alzheimer's disease may experience impaired judgment and cognitive decline, which can increase their risk for injury. Arranging the client's environment in a way that allows them to move about freely helps promote their safety and reduces the risk of accidents or falls.
D. Assign a UAP to provide the client with total personal care.
Assigning a UAP (Unlicensed Assistive Personnel) to provide the client with total personal care may be helpful in assisting with activities of daily living. However, it does not directly address the risk for injury related to impaired judgment, and the nurse should have a central role in coordinating and overseeing the client's care.
Full Explanation
Clients with early-stage Alzheimer's disease may experience impaired judgment and cognitive decline, which can increase their risk for injury. Arranging the client's environment in a way that allows them to move about freely helps promote their safety and reduces the risk of accidents or falls.
Engaging the client in regularly scheduled activities during the day is a beneficial intervention as it provides structure and stimulation for the client. However, it may not directly address the risk for injury related to impaired judgment.
Offering the client frequent reassurance that they will be safe is important to provide emotional support, but it may not be sufficient in preventing physical harm or addressing the specific nursing problem of risk for injury.
Assigning a UAP (Unlicensed Assistive Personnel) to provide the client with total personal care may be helpful in assisting with activities of daily living. However, it does not directly address the risk for injury related to impaired judgment, and the nurse should have a central role in coordinating and overseeing the client's care.
While changing a client's postoperative dressing, the nurse observes purulent drainage at the wound. Before reporting this finding to the healthcare provider, the nurse should note which of the client's laboratory values?
A. Hematocrit.
B. Platelet count.
C. Creatinine level.
D. White blood cell (WBC) count.
The presence of purulent drainage at the wound indicates a potential infection, and monitoring the client's WBC count is an important laboratory value to assess for signs of infection. An elevated WBC count, specifically an increase in the neutrophil count (neutrophilia), can indicate an active infection and provide important information for the healthcare provider when evaluating the wound. While hematocrit, platelet count, and creatinine level are essential laboratory values to assess the client's overall condition, they may not provide specific information regarding the presence of infection or purulent drainage at the wound site.
Full Explanation
The presence of purulent drainage at the wound indicates a potential infection, and monitoring the client's WBC count is an important laboratory value to assess for signs of infection. An elevated WBC count, specifically an increase in the neutrophil count (neutrophilia), can indicate an active infection and provide important information for the healthcare provider when evaluating the wound.
While hematocrit, platelet count, and creatinine level are essential laboratory values to assess the client's overall condition, they may not provide specific information regarding the presence of infection or purulent drainage at the wound site.
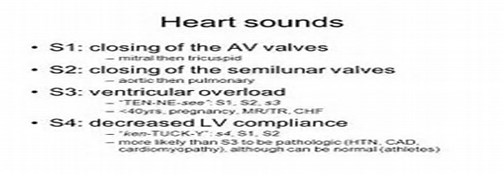
An S3 heart sound is auscultated in a client in her third trimester of pregnancy. What intervention should the nurse take?
A. Document in the client's record.
An S3 heart sound can be a normal finding during pregnancy due to increased blood volume and changes in cardiac output. It is known as a physiological S3 and is considered a benign finding in the absence of other concerning symptoms or signs. In this case, there is no immediate need for intervention or concern regarding the S3 heart sound. It is not necessary to prepare the client for an echocardiogram or limit the client's fluids based solely on the presence of an S3 heart sound in the absence of other significant symptoms or complications.
B. Prepare the client for an echocardiogram.
C. Notify the healthcare provider.
D. Limit the client's fluids.
Full Explanation
An S3 heart sound can be a normal finding during pregnancy due to increased blood volume and changes in cardiac output. It is known as a physiological S3 and is considered a benign finding in the absence of other concerning symptoms or signs.
In this case, there is no immediate need for intervention or concern regarding the S3 heart sound. It is not necessary to prepare the client for an echocardiogram or limit the client's fluids based solely on the presence of an S3 heart sound in the absence of other significant symptoms or complications.