Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse in the ICU is caring for a client who has heart failure and is receiving a dobutamine drip. The nurse should identify that which of the following findings indicates that the medication is effective?
A. Increased urine output
Reason: Dobutamine is a positive inotropic agent that increases the contractility of the heart and improves cardiac output. This leads to increased renal perfusion and urine output, which reduces the fluid overload and edema associated with heart failure. Therefore, this choice is correct.
B. Decreased blood glucose level
Reason: Dobutamine does not have a direct effect on blood glucose level. It may cause hyperglycemia as a side effect, but this is not an indication of its effectiveness. Therefore, this choice is incorrect.
C. Decreased blood pressure
Reason: Dobutamine may cause a slight decrease in blood pressure due to vasodilation, but this is not its main therapeutic effect. A significant decrease in blood pressure may indicate hypovolemia, hypotension, or shock, which are adverse effects of dobutamine. Therefore, this choice is incorrect.
D. Increased heart rate
Reason: Dobutamine also has a positive chronotropic effect, which means it increases the heart rate. However, this is not a desired outcome for a client with heart failure, as it increases the oxygen demand of the heart and may worsen the condition. Therefore, this choice is incorrect.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Custom N235 Final Summer 2023 Proctored Exam. Take the full exam now
Full Explanation
Choice A Reason: Dobutamine is a positive inotropic agent that increases the contractility of the heart and improves cardiac output. This leads to increased renal perfusion and urine output, which reduces the fluid overload and edema associated with heart failure. Therefore, this choice is correct.
Choice B Reason: Dobutamine does not have a direct effect on blood glucose level. It may cause hyperglycemia as a side effect, but this is not an indication of its effectiveness. Therefore, this choice is incorrect.
Choice C Reason: Dobutamine may cause a slight decrease in blood pressure due to vasodilation, but this is not its main therapeutic effect. A significant decrease in blood pressure may indicate hypovolemia, hypotension, or shock, which are adverse effects of dobutamine. Therefore, this choice is incorrect.
Choice D Reason: Dobutamine also has a positive chronotropic effect, which means it increases the heart rate. However, this is not a desired outcome for a client with heart failure, as it increases the oxygen demand of the heart and may worsen the condition. Therefore, this choice is incorrect.
Similar Questions
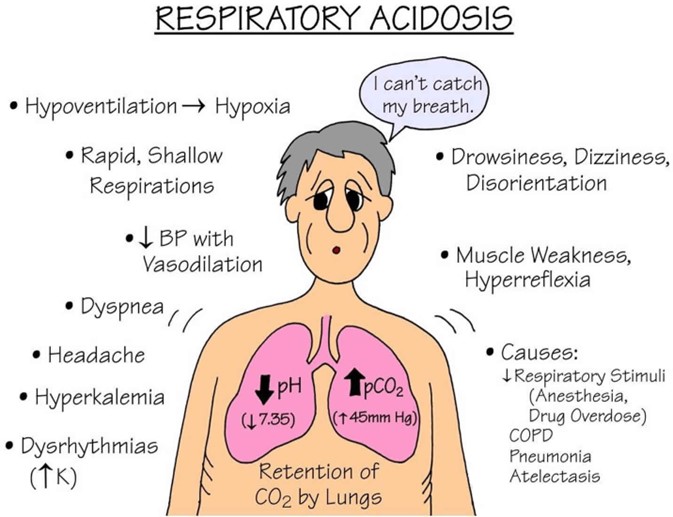
A nurse is reviewing the laboratory values of a client who has respiratory acidosis. Which of the following findings should the nurse expect?
A. PaCO2: 50 mm Hg
Reason: This choice is correct because respiratory acidosis is a condition in which the lungs cannot eliminate enough carbon dioxide (CO2) from the blood, resulting in a high level of CO2 (PaCO2) and a low level of pH. A normal PaCO2 range is 35 to 45 mm Hg, so a value of 50 mm Hg indicates respiratory acidosis.
B. HCO3: 30 mEq/L
Reason: This choice is incorrect because HCO3 (bicarbonate) is a base that helps to buffer the excess acid in the blood. In respiratory acidosis, the kidneys try to compensate by retaining more HCO3 and excreting more hydrogen ions. Therefore, a high level of HCO3 (above 26 mEq/L) would indicate a chronic or compensated respiratory acidosis, not an acute or uncompensated one.
C. pH: 7.45
Reason: This choice is incorrect because pH is a measure of the acidity or alkalinity of the blood. A normal pH range is 7.35 to 7.45, so a value of 7.45 indicates a neutral or slightly alkaline blood, not an acidic one. A low pH (below 7.35) would indicate respiratory acidosis.
D. Potassium: 3 mEq/L
Reason: This choice is incorrect because potassium is an electrolyte that helps to regulate the nerve and muscle function, as well as the fluid balance in the body. In respiratory acidosis, the increased hydrogen ions in the blood may shift into the cells in exchange for potassium, resulting in a high level of potassium (hyperkalemia). Therefore, a low level of potassium (below 3.5 mEq/L) would indicate hypokalemia, not respiratory acidosis.
Full Explanation
Choice A Reason: This choice is correct because respiratory acidosis is a condition in which the lungs cannot eliminate enough carbon dioxide (CO2) from the blood, resulting in a high level of CO2 (PaCO2) and a low level of pH. A normal PaCO2 range is 35 to 45 mm Hg, so a value of 50 mm Hg indicates respiratory acidosis.
Choice B Reason: This choice is incorrect because HCO3 (bicarbonate) is a base that helps to buffer the excess acid in the blood. In respiratory acidosis, the kidneys try to compensate by retaining more HCO3 and excreting more hydrogen ions. Therefore, a high level of HCO3 (above 26 mEq/L) would indicate a chronic or compensated respiratory acidosis, not an acute or uncompensated one.
Choice C Reason: This choice is incorrect because pH is a measure of the acidity or alkalinity of the blood. A normal pH range is 7.35 to 7.45, so a value of 7.45 indicates a neutral or slightly alkaline blood, not an acidic one. A low pH (below 7.35) would indicate respiratory acidosis.
Choice D Reason: This choice is incorrect because potassium is an electrolyte that helps to regulate the nerve and muscle function, as well as the fluid balance in the body. In respiratory acidosis, the increased hydrogen ions in the blood may shift into the cells in exchange for potassium, resulting in a high level of potassium (hyperkalemia).
Therefore, a low level of potassium (below 3.5 mEq/L) would indicate hypokalemia, not respiratory acidosis.
A nurse in the emergency department is caring for a client who has sustained a head injury. The nurse notes the client's IV fluids are infusing at 125 mL/hr. Which of the following is an appropriate action by the nurse?
A. Slow the rate to 50 mL/hr.
Reason: This choice is incorrect because slowing the rate to 50 mL/hr may not be enough to prevent cerebral edema, which is a common complication of head injury. Cerebral edema is a swelling of the brain tissue due to increased fluid accumulation. It can cause increased intracranial pressure (ICP), which can lead to brain damage or death. Therefore, the nurse should limit the fluid intake of the client with head injury to avoid worsening the condition.
B. Increase the rate to 250 mL/hr.
Reason: This choice is incorrect because increasing the rate to 250 mL/hr may cause fluid overload, which can also increase the ICP and worsen the cerebral edema. Fluid overload is a condition in which the body has too much fluid, which can impair the function of the heart, lungs, and kidneys. Therefore, the nurse should avoid giving too much fluid to the client with head injury.
C. Slow the rate to 20 mL/hr.
Reason: Reducing the infusion to 20 mL/hr is excessively low and may cause hypotension or inadequate maintenance of vascular access and medication delivery. Such a drastic decrease could impair perfusion to injured brain tissue and is not an appropriate independent nursing action without a specific order.
D. Continue the rate at 125 mL/hr.
Reason: Maintaining the current prescribed infusion rate avoids abrupt volume shifts that could alter intracranial pressure. The nurse should monitor neurologic status and vital signs, ensure the IV is patent, and follow provider orders; only change the rate when clinically indicated or when directed by the prescriber.
Full Explanation
Choice A Reason: This choice is incorrect because slowing the rate to 50 mL/hr may not be enough to prevent cerebral edema, which is a common complication of head injury. Cerebral edema is a swelling of the brain tissue due to increased fluid accumulation. It can cause increased intracranial pressure (ICP), which can lead to brain damage or death. Therefore, the nurse should limit the fluid intake of the client with head injury to avoid worsening the condition.
Choice B Reason: This choice is incorrect because increasing the rate to 250 mL/hr may cause fluid overload, which can also increase the ICP and worsen the cerebral edema. Fluid overload is a condition in which the body has too much fluid, which can impair the function of the heart, lungs, and kidneys. Therefore, the nurse should avoid giving too much fluid to the client with head injury.
Choice C reason: Reducing the infusion to 20 mL/hr is excessively low and may cause hypotension or inadequate maintenance of vascular access and medication delivery. Such a drastic decrease could impair perfusion to injured brain tissue and is not an appropriate independent nursing action without a specific order.
Choice D reason: Maintaining the current prescribed infusion rate avoids abrupt volume shifts that could alter intracranial pressure. The nurse should monitor neurologic status and vital signs, ensure the IV is patent, and follow provider orders; only change the rate when clinically indicated or when directed by the prescriber.
A nurse in an emergency department is caring for a client who has a sucking chest wound resulting from a gunshot. The client has a blood pressure of 100/60 mm Hg, a weak pulse rate of 118/min, and a respiratory rate of 40/min. Which of the following actions should the nurse take?
A. Prepare to insert a central line.
Reason: This choice is incorrect because inserting a central line is not a priority action for a client who has a sucking chest wound. A central line is a catheter that is inserted into a large vein in the neck, chest, or groin to administer fluids, medications, or blood products. It may be indicated for clients who have hypovolemia, sepsis, or shock, but it does not address the underlying cause of the client's respiratory distress.
B. Remove the dressing to inspect the wound.
Reason: This choice is incorrect because removing the dressing to inspect the wound may worsen the client's condition. A sucking chest wound is an open wound in the chest wall that allows air to enter and exit the pleural cavity with each breath. This creates a positive pressure in the pleural space that collapses the lung on the affected side and shifts the mediastinum to the opposite side, impairing the ventilation and circulation of both lungs. Therefore, the nurse should apply an occlusive dressing that covers three sides of the wound and allows air to escape but not enter the pleural cavity. Removing the dressing may allow more air to enter and increase the risk of tension pneumothorax, which is a life-threatening complication.
C. Administer oxygen via nasal cannula.
Reason: This choice is correct because administering oxygen via nasal cannula may help to improve the client's oxygenation and ventilation. A nasal cannula is a device that delivers oxygen through two prongs that fit into the nostrils. It can provide oxygen at low flow rates (1 to 6 L/min) and low concentrations (24 to 44 percent). The nurse should monitor the client's respiratory rate, pulse oximetry, and arterial blood gases to assess the effectiveness of oxygen therapy.
D. Raise the foot of the bed to a 90° angle.
Reason: This choice is incorrect because raising the foot of the bed to a 90° angle may worsen the client's respiratory distress. This position may increase the pressure on the diaphragm and reduce the lung expansion. It may also decrease the venous return and cardiac output, leading to hypotension and shock. Therefore, the nurse should position the client in a semi-Fowler's position (30 to 45° angle) or high-Fowler's position (60 to 90° angle) to facilitate breathing and prevent further complications.
Full Explanation
Choice A Reason: This choice is incorrect because inserting a central line is not a priority action for a client who has a sucking chest wound. A central line is a catheter that is inserted into a large vein in the neck, chest, or groin to administer fluids, medications, or blood products. It may be indicated for clients who have hypovolemia, sepsis, or shock, but it does not address the underlying cause of the client's respiratory distress.
Choice B Reason: This choice is incorrect because removing the dressing to inspect the wound may worsen the client's condition. A sucking chest wound is an open wound in the chest wall that allows air to enter and exit the pleural cavity with each breath. This creates a positive pressure in the pleural space that collapses the lung on the affected side and shifts the mediastinum to the opposite side, impairing the ventilation and circulation of both lungs. Therefore, the nurse should apply an occlusive dressing that covers three sides of the wound and allows air to escape but not enter the pleural cavity. Removing the dressing may allow more air to enter and increase the risk of tension pneumothorax, which is a life-threatening complication.
Choice C Reason: This choice is correct because administering oxygen via nasal cannula may help to improve the client's oxygenation and ventilation. A nasal cannula is a device that delivers oxygen through two prongs that fit into the nostrils. It can provide oxygen at low flow rates (1 to 6 L/min) and low concentrations (24 to 44 percent). The nurse should monitor the client's respiratory rate, pulse oximetry, and arterial blood gases to assess the effectiveness of oxygen therapy.
Choice D Reason: This choice is incorrect because raising the foot of the bed to a 90° angle may worsen the client's respiratory distress. This position may increase the pressure on the diaphragm and reduce the lung expansion. It may also decrease the venous return and cardiac output, leading to hypotension and shock. Therefore, the nurse should position the client in a semi-Fowler's position (30 to 45° angle) or high-Fowler's position (60 to 90° angle) to facilitate breathing and prevent further complications.
