Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is assessing a client in the oliguric phase of acute kidney injury. Which of the following findings should the nurse expect?
A. Hypomagnesemia
Reason: This choice is incorrect because hypomagnesemia is not a common finding in the oliguric phase of acute kidney injury. Hypomagnesemia is a condition in which the serum magnesium level is lower than normal (less than 1.5 mEq/L). It may be caused by various factors such as malnutrition, diarrhea, diuretics, or alcohol abuse. It may cause symptoms such as muscle weakness, tremors, tetany, or cardiac arrhythmias.
B. Hyperkalemia
Reason: This choice is correct because hyperkalemia is a common finding in the oliguric phase of acute kidney injury. Hyperkalemia is a condition in which the serum potassium level is higher than normal (more than 5 mEq/L). It may be caused by reduced renal excretion of potassium due to decreased urine output (oliguria). It may cause symptoms such as muscle weakness, paresthesia, bradycardia, or cardiac arrest.
C. Decreased creatinine level
Reason: This choice is incorrect because decreased creatinine level is not a common finding in the oliguric phase of acute kidney injury. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys and excreted in urine. A normal creatinine level ranges from 0.6 to 1.2 mg/dL for men and 0.5 to 1.1 mg/dL for women. In acute kidney injury, creatinine level usually increases due to reduced renal function and impaired clearance of creatinine.
D. Increased glomerular filtration rate (GFR)
Reason: This choice is incorrect because increased glomerular filtration rate (GFR) is not a common finding in the oliguric phase of acute kidney injury. GFR is a measure of how well the kidneys filter blood and remove waste products. A normal GFR range is 90,to 120 mL/min/1.73 m2. In acute kidney injury, GFR usually decreases due to reduced blood flow,to,the kidneys or damage to the glomeruli, which are the tiny blood vessels that filter blood in the kidneys.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Custom N235 Final Summer 2023 Proctored Exam. Take the full exam now
Full Explanation
Choice A Reason: This choice is incorrect because hypomagnesemia is not a common finding in the oliguric phase of acute kidney injury. Hypomagnesemia is a condition in which the serum magnesium level is lower than normal (less than 1.5 mEq/L). It may be caused by various factors such as malnutrition, diarrhea, diuretics, or alcohol abuse. It may cause symptoms such as muscle weakness, tremors, tetany, or cardiac arrhythmias.
Choice B Reason: This choice is correct because hyperkalemia is a common finding in the oliguric phase of acute kidney injury. Hyperkalemia is a condition in which the serum potassium level is higher than normal (more than 5 mEq/L). It may be caused by reduced renal excretion of potassium due to decreased urine output (oliguria). It may cause symptoms such as muscle weakness, paresthesia, bradycardia, or cardiac arrest.
Choice C Reason: This choice is incorrect because decreased creatinine level is not a common finding in the oliguric phase of acute kidney injury. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys and excreted in urine. A normal creatinine level ranges from 0.6 to 1.2 mg/dL for men and 0.5 to 1.1 mg/dL for women. In acute kidney injury, creatinine level usually increases due to reduced renal function and impaired clearance of creatinine.
Choice D Reason: This choice is incorrect because increased glomerular filtration rate (GFR) is not a common finding in the oliguric phase of acute kidney injury. GFR is a measure of how well
the kidneys filter blood and remove waste products.
A normal GFR range is 90,to 120 mL/min/1.73 m2. In acute kidney injury, GFR usually decreases due to reduced blood flow,to,the kidneys or damage to the glomeruli, which are the tiny blood vessels that filter blood in the kidneys.
Similar Questions
A nurse is caring for a client who has increased intracranial pressure. Which of the following interventions should the nurse take?
A. Provide a brightly lit environment.
Reason: This choice is incorrect because providing a brightly lit environment may stimulate the client and increase the intracranial pressure. A brightly lit environment is an environment that has a high level of illumination or brightness. It may be used for clients who have depression, seasonal affective disorder, or insomnia, but it does not help to reduce the intracranial pressure.
B. Teach controlled coughing and deep breathing.
Reason: This choice is incorrect because teaching controlled coughing and deep breathing may increase the intrathoracic pressure and increase the intracranial pressure. Controlled coughing and deep breathing are techniques that help to clear the airway and improve lung expansion. They may be used for clients who have respiratory infections, chronic obstructive pulmonary disease, or postoperative complications, but they do not help to reduce the intracranial pressure.
C. Encourage a minimum intake of 2000 mL (67.5 oz) of clear fluids per day.
Reason: This choice is incorrect because encouraging a minimum intake of 2000 mL (67.5 oz) of clear fluids per day may cause fluid overload and increase the intracranial pressure. Fluid overload is a condition in which the body has too much fluid, which can impair the function of the heart, lungs, and kidneys. Therefore, restricting fluid intake and using diuretics may be indicated for clients who have increased intracranial pressure.
D. Elevate the head of the bed 20°.
Reason: This choice is correct because elevating the head of the bed 20° may help to improve the venous drainage and decrease the intracranial pressure. As explained above, positioning the client in a semi-Fowler's or high-Fowler's position can facilitate breathing and prevent further complications. However, elevating the head of the bed more than 30° may decrease the cerebral perfusion pressure (CPP), which is the difference between the mean arterial pressure (MAP) and the intracranial pressure (ICP). A normal CPP range is 70 to 100 mm Hg, and a low CPP (<50 mm Hg) can cause cerebral ischemia, herniation, or death. Therefore, elevating the head of the bed to a moderate angle (20°) may be optimal for clients who have increased ICP.
Full Explanation
Choice A Reason: This choice is incorrect because providing a brightly lit environment may stimulate the client and increase the intracranial pressure. A brightly lit environment is an environment that has a high level of illumination or brightness. It may be used for clients who have depression, seasonal affective disorder, or insomnia, but it does not help to reduce the intracranial pressure.
Choice B Reason: This choice is incorrect because teaching controlled coughing and deep breathing may increase the intrathoracic pressure and increase the intracranial pressure. Controlled coughing and deep breathing are techniques that help to clear the airway and improve lung expansion. They may be used for clients who have respiratory infections, chronic obstructive pulmonary disease, or postoperative complications, but they do not help to reduce the intracranial pressure.
Choice C Reason: This choice is incorrect because encouraging a minimum intake of 2000 mL (67.5 oz) of clear fluids per day may cause fluid overload and increase the intracranial pressure. Fluid overload is a condition in which the body has too much fluid, which can impair the function of the heart, lungs, and kidneys. Therefore, restricting fluid intake and using diuretics may be indicated for clients who have increased intracranial pressure.
Choice D Reason: This choice is correct because elevating the head of the bed 20° may help to improve the venous drainage and decrease the intracranial pressure. As explained above, positioning the client in a semi-Fowler's or high-Fowler's position can facilitate breathing and prevent further complications. However, elevating the head of the bed more than 30° may decrease the cerebral perfusion pressure (CPP), which is the difference between the mean arterial pressure (MAP) and the intracranial pressure (ICP). A normal CPP range is 70 to 100 mm Hg, and a low CPP (<50 mm Hg) can cause cerebral ischemia, herniation, or death. Therefore, elevating the head of the bed to a moderate angle (20°) may be optimal for clients who have increased ICP.
A client who is having burn debridement states, "You are the worst nurse I have ever seen. All you do is hurt me." Which of the following responses should the nurse make?
A. "That's a hurtful thing to say."
Reason: This choice is incorrect because it reflects the nurse's feelings rather than focusing on the client's needs. Saying "That's a hurtful thing to say" may make the client feel guilty or defensive, and it does not address the underlying cause of the client's anger or frustration.
B. "Why would you say such a thing?"
Reason: This choice is incorrect because it sounds accusatory and confrontational rather than empathetic and supportive. Asking "Why would you say such a thing?" may make the client feel judged or criticized, and it does not explore the client's feelings or concerns.
C. "Well, that's your opinion."
Reason: This choice is incorrect because it dismisses the client's feelings rather than acknowledging them. Saying "Well, that's your opinion" may make the client feel ignored or invalidated, and it does not show respect or compassion for the client.
D. "Tell me more about that."
Reason: This choice is correct because it invites the client to express their feelings and concerns rather than shutting them down. Saying "Tell me more about that" may make the client feel heard and understood, and it may help to identify the source of their anger or frustration. The nurse can then use therapeutic communication skills such as active listening, reflecting, clarifying, or validating to establish rapport and trust with the client.
Full Explanation
Choice A Reason: This choice is incorrect because it reflects the nurse's feelings rather than focusing on the client's needs. Saying "That's a hurtful thing to say" may make the client feel guilty or defensive, and it does not address the underlying cause of the client's anger or frustration.
Choice B Reason: This choice is incorrect because it sounds accusatory and confrontational rather than empathetic and supportive. Asking "Why would you say such a thing?" may make the client feel judged or criticized, and it does not explore the client's feelings or concerns.
Choice C Reason: This choice is incorrect because it dismisses the client's feelings rather than acknowledging them. Saying "Well, that's your opinion" may make the client feel ignored or invalidated, and it does not show respect or compassion for the client.
Choice D Reason: This choice is correct because it invites the client to express their feelings and concerns rather than shutting them down. Saying "Tell me more about that" may make the client feel heard and understood, and it may help to identify the source of their anger or frustration. The nurse can then use therapeutic communication skills such as active listening, reflecting, clarifying, or validating to establish rapport and trust with the client.
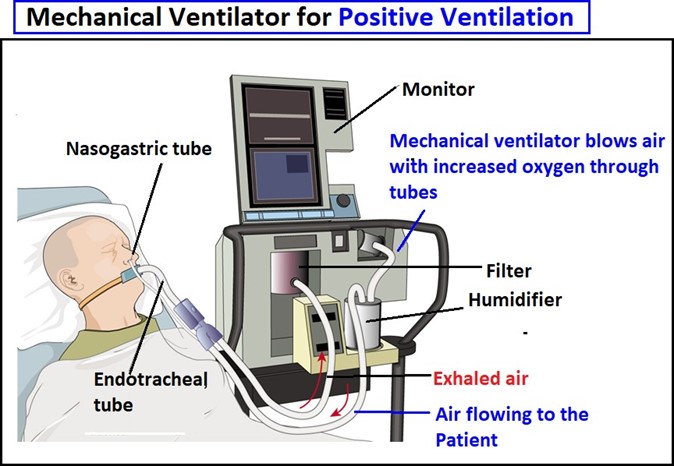
A nurse is caring for a client who is receiving positive-pressure mechanical ventilation. Which of the following interventions should the nurse implement to prevent complications? (Select all that apply.)
A. Verify the prescribed ventilator settings daily.
Choice A Reason: This choice is correct because verifying the prescribed ventilator settings daily is an important intervention to ensure that the client is receiving adequate ventilation and oxygenation. The ventilator settings include parameters such as tidal volume, respiratory rate, fraction of inspired oxygen (FiO2), positive end-expiratory pressure (PEEP), and peak inspiratory pressure (PIP). The nurse should check that the settings match the prescription and report any changes or alarms to the provider.
B. Apply restraints if the client becomes agitated.
Choice B Reason: This choice is incorrect because applying restraints if the client becomes agitated is not a recommended intervention to prevent complications. Restraints may cause injury, infection, or psychological distress to the client and increase the risk of ventilator-associated pneumonia (VAP). The nurse should use alternative methods to manage agitation, such as sedation, analgesia, or environmental modification.
C. Administer pantoprazole as prescribed.
Choice C Reason: This choice is correct because administering pantoprazole as prescribed is an important intervention to prevent complications. Pantoprazole is a proton pump inhibitor (PPI) that reduces the production of stomach acid and prevents gastroesophageal reflux disease (GERD) and stress ulcers. These conditions can cause aspiration, bleeding, or infection in clients who are receiving mechanical ventilation.
D. Reposition the endotracheal tube to the opposite side of the mouth daily.
Choice D Reason: This choice is incorrect because repositioning the endotracheal tube to the opposite side of the mouth daily is not a recommended intervention to prevent complications. Repositioning the endotracheal tube may cause trauma, bleeding, or displacement of the tube, which can compromise the airway and ventilation of the client. The nurse should secure the tube with tape or a device and check its position regularly using chest x-ray or end-tidal CO2 monitoring.
E. Elevate the head of the bed to at least 30°.
Choice E Reason: This choice is correct because elevating the head of the bed to at least 30° is an important intervention to prevent complications. Elevatin the head of the bed helps to reduce the risk of aspiration, which is the inhalation of gastric contents or secretions into the lungs. Aspiration can cause pneumonia, atelectasis, or respiratory failure in clients who are receiving mechanical ventilation.
Full Explanation
Choice A Reason: This choice is correct because verifying the prescribed ventilator settings daily is an important intervention to ensure that the client is receiving adequate ventilation and oxygenation. The ventilator settings include parameters such as tidal volume, respiratory rate, fraction of inspired oxygen (FiO2), positive end-expiratory pressure (PEEP), and peak inspiratory pressure (PIP). The nurse should check that the settings match the prescription and report any changes or alarms to the provider.
Choice B Reason: This choice is incorrect because applying restraints if the client becomes agitated is not a recommended intervention to prevent complications. Restraints may cause injury, infection, or psychological distress to the client and increase the risk of ventilator-associated pneumonia (VAP). The nurse should use alternative methods to manage agitation, such as sedation, analgesia, or environmental modification.
Choice C Reason: This choice is correct because administering pantoprazole as prescribed is an important intervention to prevent complications. Pantoprazole is a proton pump inhibitor (PPI) that reduces the production of stomach acid and prevents gastroesophageal reflux disease (GERD) and stress ulcers. These conditions can cause aspiration, bleeding, or infection in clients who are receiving mechanical ventilation.
Choice D Reason: This choice is incorrect because repositioning the endotracheal tube to the opposite side of the mouth daily is not a recommended intervention to prevent complications. Repositioning the endotracheal tube may cause trauma, bleeding, or displacement of the tube, which can compromise the airway and ventilation of the client. The nurse should secure the tube with tape or a device and check its position regularly using chest x-ray or end-tidal CO2 monitoring.
Choice E Reason: This choice is correct because elevating the head of the bed to at least 30° is an important intervention to prevent complications. Elevatin the head of the bed helps to reduce the risk of aspiration, which is the inhalation of gastric contents or secretions into the lungs. Aspiration can cause pneumonia, atelectasis, or respiratory failure in clients who are receiving mechanical ventilation.