Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is assessing a client who has right-sided heart failure.
Which of the following assessment findings should the nurse expect to find?
A. Poor skin turgor.
Choice A is incorrect because poor skin turgor is not a common symptom of right-sided heart failure.
B. Pitting edema.
Pitting edema is a common and obvious symptom of right-sided heart failure. This occurs when fluid retention causes swelling in the lower limbs and sometimes the abdomen.
C. Oliguria.
Choice C is incorrect because oliguria, or decreased urine output, is not a common symptom of right-sided heart failure.
D. S4 galloping heart sounds.
Choice D is incorrect because S4 galloping heart sounds are not a common symptom of right-sided heart failure.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Adult Medical Surgical 2019 Proctored Exam. Take the full exam now
Full Explanation
Pitting edema is a common and obvious symptom of right-sided heart failure.

This occurs when fluid retention causes swelling in the lower limbs and sometimes the abdomen.
Choice A is incorrect because poor skin turgor is not a common symptom of right-sided heart failure.
Choice C is incorrect because oliguria, or decreased urine output, is not a common symptom of right-sided heart failure.
Choice D is incorrect because S4 galloping heart sounds are not a common symptom of right-sided heart failure.
Similar Questions
A nurse on a medical unit is planning care for a group of clients.
Which of the following clients should the nurse attend to first?
A. A client who has chronic obstructive pulmonary disease and an oxygen saturation of 89%.
The client with chronic obstructive pulmonary disease and an oxygen saturation of 89% may require oxygen therapy or other interventions to improve respiratory function, but the situation is not immediately life-threatening.
B. A client who has thrombocytopenia and reports a nosebleed.
The nurse should attend to the client who has thrombocytopenia and reports a nosebleed first. Thrombocytopenia is a condition characterized by low platelet count, which increases the risk of bleeding. A nosebleed can be a sign of significant bleeding, and it is important for the nurse to assess the severity and take appropriate action to stop the bleeding and prevent further complications. Although the other clients also require nursing care, their conditions are not as urgent as the client with thrombocytopenia and a nosebleed.
C. A client who has left-sided paralysis and slurred speech from a prior stroke.
The client with left-sided paralysis and slurred speech from a prior stroke may require ongoing care and rehabilitation, but there is no indication of an acute change in their condition.
D. A client who has multiple sclerosis and reports ataxia and vertigo.
The client with multiple sclerosis and ataxia and vertigo may require assistance with mobility and balance, but their symptoms do not pose an immediate threat to their health.
Full Explanation
The nurse should attend to the client who has thrombocytopenia and reports a nosebleed first.

Thrombocytopenia is a condition characterized by low platelet count, which increases the risk of bleeding.
A nosebleed can be a sign of significant bleeding, and it is important for the nurse to assess the severity and take appropriate action to stop the bleeding and prevent further complications.
Although the other clients also require nursing care, their conditions are not as urgent as the client with thrombocytopenia and a nosebleed.
The client with chronic obstructive pulmonary disease and an oxygen saturation of 89% may require oxygen therapy or other interventions to improve respiratory function, but the situation is not immediately life-threatening.
The client with left-sided paralysis and slurred speech from a prior stroke may require ongoing care and rehabilitation, but there is no indication of an acute change in their condition.
The client with multiple sclerosis and ataxia and vertigo may require assistance with mobility and balance, but their symptoms do not pose an immediate threat to their health.
A nurse is caring for a client who is postoperative following an endoscopy with moderate (conscious) sedation.
Which of the following assessment findings is the nurse's priority?
A. Level of pain.
Choice A is incorrect because while pain management is important, it is not the nurse’s priority in this situation.
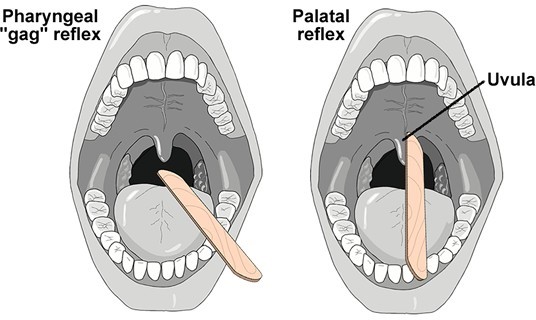
B. Gag reflex.
The nurse’s priority should be to assess the client’s gag reflex. After an endoscopy with moderate (conscious) sedation, it is important to ensure that the client’s gag reflex has returned before allowing them to eat or drink.
C. Warmth of extremities.
Choice C is incorrect because the warmth of extremities is not the nurse’s priority in this situation.
D. Temperature.
Choice D is incorrect because temperature is not the nurse’s priority in this situation.
Full Explanation
The nurse’s priority should be to assess the client’s gag reflex.
After an endoscopy with moderate (conscious) sedation, it is important to ensure that the client’s gag reflex has returned before allowing them to eat or drink.
Choice A is incorrect because while pain management is important, it is not the nurse’s priority in this situation.
Choice C is incorrect because the warmth of extremities is not the nurse’s priority in this situation.
Choice D is incorrect because temperature is not the nurse’s priority in this situation.
Exhibit 1 Exhibit 2 Graphic Record Blood pressure 176/122 mm Hg Heart rate 136/min Respiratory rate 32/min Exhibit 3 O2 saturation 88%.
A nurse in the emergency department is caring for a client who was involved in an explosion.
Which of the following actions should the nurse plan to take first? (Click on the "Exhibit" button for additional information about the client.
A. Obtain an ECG.
Choice A is incorrect because while obtaining an ECG may be important, it is not the nurse’s first priority in this situation.
B. Calculate the extent of burns using the rule of nines.
Choice B is incorrect because while calculating the extent of burns using the rule of nines may be important, it is not the nurse’s first priority in this situation.
C. Notify the Rapid Response Team.
The nurse should plan to notify the Rapid Response Team first. The client’s blood pressure is elevated, heart rate is high, respiratory rate is high, and oxygen saturation is low. These are all signs of potential instability and the Rapid Response Team should be notified immediately.
D. Initiate peripheral IV access.
Choice D is incorrect because while initiating peripheral IV access may be important, it is not the nurse’s first priority in this situation.
Full Explanation
The nurse should plan to notify the Rapid Response Team first.
The client’s blood pressure is elevated, heart rate is high, respiratory rate is high, and oxygen saturation is low.
These are all signs of potential instability and the Rapid Response Team should be notified immediately.
Choice A is incorrect because while obtaining an ECG may be important, it is not the nurse’s first priority in this situation.
Choice B is incorrect because while calculating the extent of burns using the rule of nines may be important, it is not the nurse’s first priority in this situation.
Choice D is incorrect because while initiating peripheral IV access may be important, it is not the nurse’s first priority in this situation.