Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is assessing a client's cranial nerves as part of a neurological examination. Which of the following actions should the nurse take to assess cranial nerve III?
A. Eliciting the gag reflex
Eliciting the gag reflex is a way to assess cranial nerve IX (glossopharyngeal) and X (vagus), which are responsible for the sensation and motor function of the pharynx and larynx.
B. Testing visual acuity
Testing visual acuity is a way to assess cranial nerve II (optic), which is responsible for the sense of vision.
C. Observing for facial symmetry
Observing for facial symmetry is a way to assess cranial nerve VII (facial), which is responsible for the motor function of the facial muscles and the sensation of taste.
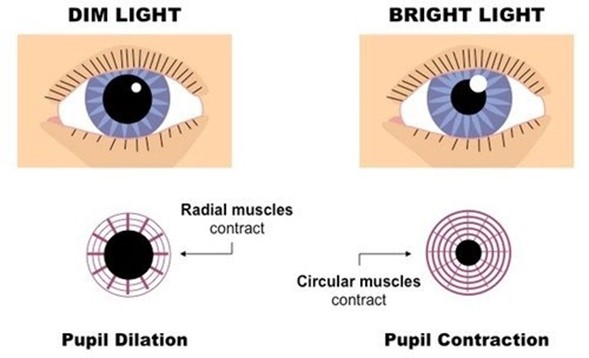
D. Checking the pupillary response to light
Checking the pupillary response to light is a way to assess cranial nerve III (oculomotor), which is responsible for the motor function of most of the eye muscles, including those that control pupil size and lens shape.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Custom N235 Final Summer 2023 Proctored Exam. Take the full exam now
Full Explanation
Choice A: Eliciting the gag reflex is a way to assess cranial nerve IX (glossopharyngeal) and X (vagus), which are responsible for the sensation and motor function of the pharynx and larynx.
Choice B: Testing visual acuity is a way to assess cranial nerve II (optic), which is responsible for the sense of vision.
Choice C: Observing for facial symmetry is a way to assess cranial nerve VII (facial), which is responsible for the motor function of the facial muscles and the sensation of taste.
Choice D: Checking the pupillary response to light is a way to assess cranial nerve III (oculomotor), which is responsible for the motor function of most of the eye muscles, including those that control pupil size and lens shape.
Similar Questions
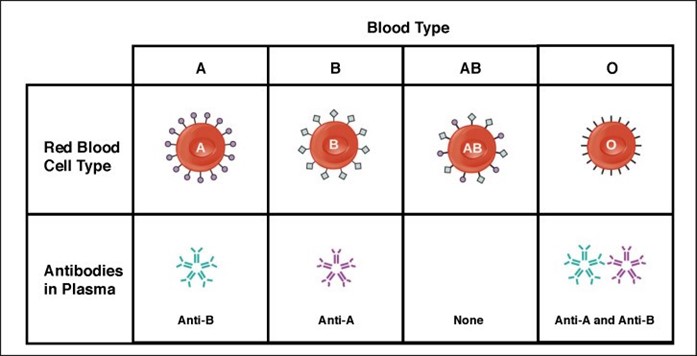
A nurse is preparing to administer blood to a client. The unit of blood on hand is type B, and the client has type AB blood. Which of the following actions should the nurse take?
A. Contact the provider for further orders.
Contacting the provider for further orders is not necessary, because the client has type AB blood, which is compatible with any other blood type. The client can receive type B blood without any adverse reactions.
B. Notify the blood bank of the discrepancy.
Notifying the blood bank of the discrepancy is not required, because there is no discrepancy. The blood bank sent the correct type of blood for the client, according to their blood type.
C. Administer the blood as ordered.
Administering the blood as ordered is the correct action, because type B blood is compatible with type AB blood. The client will not have any transfusion reactions or complications from receiving this type of blood.
D. Complete an incident report.
Completing an incident report is not appropriate, because there is no incident. The nurse did not make any error or mistake in administering the blood to the client. There is no need to document or report anything unusual.
Full Explanation
Choice A: Contacting the provider for further orders is not necessary, because the client has type AB blood, which is compatible with any other blood type. The client can receive type B blood without any adverse reactions.
Choice B: Notifying the blood bank of the discrepancy is not required, because there is no discrepancy. The blood bank sent the correct type of blood for the client, according to their blood type.
Choice C: Administering the blood as ordered is the correct action, because type B blood is compatible with type AB blood. The client will not have any transfusion reactions or complications from receiving this type of blood.
Choice D: Completing an incident report is not appropriate, because there is no incident. The nurse did not make any error or mistake in administering the blood to the client. There is no need to document or report anything unusual.
The nurse in a trauma unit has received a report on a client who has multiple injuries following a motor vehicle crash. Which of the following actions should the nurse plan to take first?
A. Evaluate chest expansion.
Evaluating chest expansion is the first action that the nurse should take, because it assesses the client's respiratory status and potential for pneumothorax, which is a life-threatening condition that can result from chest trauma. The nurse should compare the movement of both sides of the chest and listen for breath sounds.
B. Check pupillary response to light.
Checking pupillary response to light is an important action, but not the first one, because it assesses the client's neurological status and potential for brain injury. The nurse should observe the size, shape, and symmetry of the pupils and their reaction to light.
C. Check the client's response to questions about place and time.
Checking the client's response to questions about place and time is another important action, but not the first one, because it assesses the client's level of consciousness and orientation. The nurse should ask the client simple questions such as their name, date, and location.
D. Assess the capillary refill.
Assessing the capillary refill is a less important action, and not the first one, because it assesses the client's peripheral circulation and tissue perfusion. The nurse should press on the client's nail beds or fingertips and observe how quickly the color returns.
Full Explanation
Choice A: Evaluating chest expansion is the first action that the nurse should take, because it assesses the client's respiratory status and potential for pneumothorax, which is a life-threatening condition that can result from chest trauma. The nurse should compare the movement of both sides of the chest and listen for breath sounds.
Choice B: Checking pupillary response to light is an important action, but not the first one, because it assesses the client's neurological status and potential for brain injury. The nurse should observe the size, shape, and symmetry of the pupils and their reaction to light.
Choice C: Checking the client's response to questions about place and time is another important action, but not the first one, because it assesses the client's level of consciousness and orientation. The nurse should ask the client simple questions such as their name, date, and location.
Choice D: Assessing the capillary refill is a less important action, and not the first one, because it assesses the client's peripheral circulation and tissue perfusion. The nurse should press on the client's nail beds or fingertips and observe how quickly the color returns.
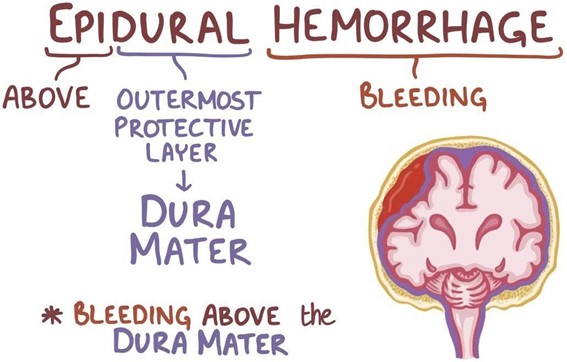
A nurse in the emergency department is caring for a client who has an epidural hematoma following a motor-vehicle crash. Which of the following is an expected finding for this client?
A. Drainage of clear fluid from the ears
Drainage of clear fluid from the ears is not an expected finding for a client who has an epidural hematoma, but rather a sign of a basilar skull fracture, which is a different type of head injury. The clear fluid is cerebrospinal fluid (CSF), which leaks from the brain through the fractured skull.
B. Alternating periods of alertness and unconsciousness
Alternating periods of alertness and unconsciousness is an expected finding for a client who has an epidural hematoma, because it indicates a rapid increase in intracranial pressure (ICP) due to bleeding between the dura mater and the skull. The client may have a brief loss of consciousness at the time of injury, followed by a lucid interval, and then a rapid deterioration of mental status.
C. Narrowing pulse pressure
Narrowing pulse pressure is not an expected finding for a client who has an epidural hematoma, but rather a sign of increased ICP due to any cause. Pulse pressure is the difference between systolic and diastolic blood pressure. As ICP rises, it compresses the brainstem and causes bradycardia and hypertension, resulting in a decreased pulse pressure.
D. Extensive bruising in the mastoid area
Extensive bruising in the mastoid area is not an expected finding for a client who has an epidural hematoma, but rather a sign of a basilar skull fracture, which is a different type of head injury. The bruising is also known as Batle's sign, and it occurs due to blood pooling behind the ear.
Full Explanation
Choice A: Drainage of clear fluid from the ears is not an expected finding for a client who has an epidural hematoma, but rather a sign of a basilar skull fracture, which is a different type of head injury. The clear fluid is cerebrospinal fluid (CSF), which leaks from the brain through the fractured skull.
Choice B: Alternating periods of alertness and unconsciousness is an expected finding for a client who has an epidural hematoma, because it indicates a rapid increase in intracranial pressure (ICP) due to bleeding between the dura mater and the skull. The client may have a brief loss of consciousness at the time of injury, followed by a lucid interval, and then a rapid deterioration of mental status.
Choice C: Narrowing pulse pressure is not an expected finding for a client who has an epidural hematoma, but rather a sign of increased ICP due to any cause. Pulse pressure is the difference between systolic and diastolic blood pressure. As ICP rises, it compresses the brainstem and causes bradycardia and hypertension, resulting in a decreased pulse pressure.
Choice D: Extensive bruising in the mastoid area is not an expected finding for a client who has an epidural hematoma, but rather a sign of a basilar skull fracture, which is a different type of head injury. The bruising is also known as Batle's sign, and it occurs due to blood pooling behind the ear.