Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
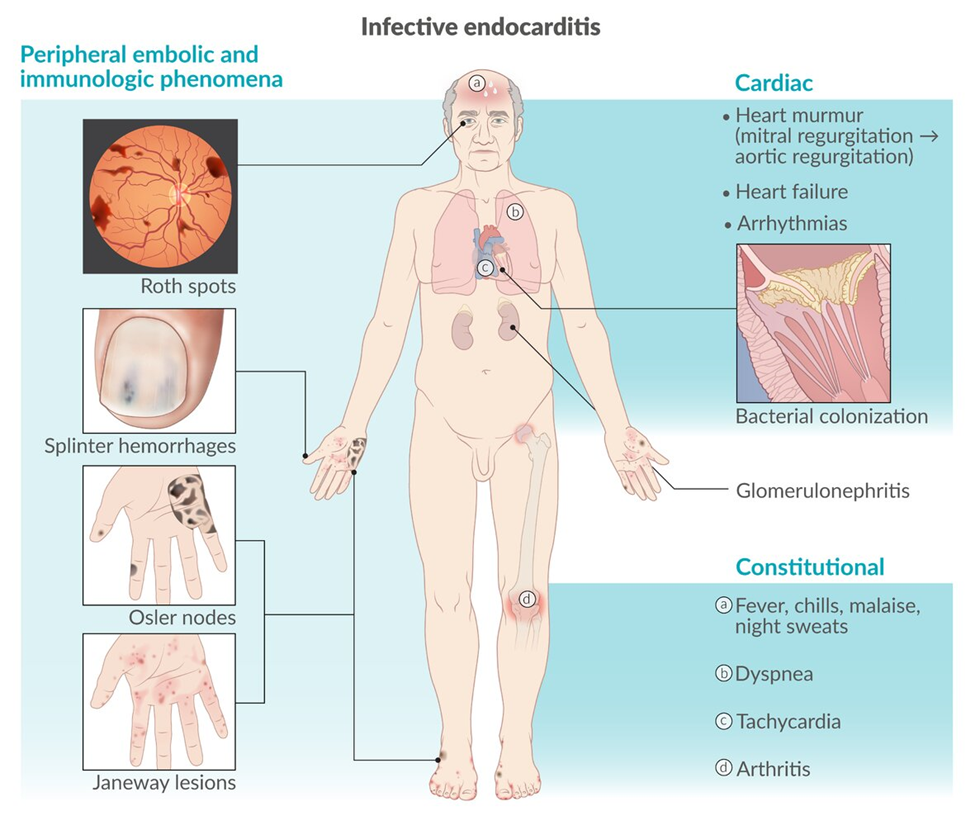
A nurse is assessing a toddler who has infective endocarditis. Which of the following findings should the nurse expect?
A. New heart murmur
New heart murmurThis is a common finding in infective endocarditis due to damage to the heart valves caused by the infection. The infection can lead to the development of new heart murmurs or changes in existing ones as the valves become affected.
B. Weight gain
Weight gainWeight gain is not typically associated with infective endocarditis. In fact, individuals with infective endocarditis may experience weight loss due to symptoms such as fever, loss of appetite, and malaise.
C. Bradycardia
Bradycardia Bradycardia, or a slow heart rate, is not a typical finding in infective endocarditis. In many cases, individuals with infective endocarditis may actually present with tachycardia (rapid heart rate) due to fever and the body's response to infection.
D. Decreased body temperature
Decreased body temperatureInfective endocarditis is often associated with fever, which would lead to an elevated body temperature rather than a decreased one.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Nursing Care Of Children Proctored Exam. Take the full exam now
Full Explanation
A. New heart murmur
This is a common finding in infective endocarditis due to damage to the heart valves caused by the infection. The infection can lead to the development of new heart murmurs or changes in existing ones as the valves become affected.
B. Weight gain
Weight gain is not typically associated with infective endocarditis. In fact, individuals with infective endocarditis may experience weight loss due to symptoms such as fever, loss of appetite, and malaise.
C. Bradycardia
Bradycardia, or a slow heart rate, is not a typical finding in infective endocarditis. In many cases, individuals with infective endocarditis may actually present with tachycardia (rapid heart rate) due to fever and the body's response to infection.
D. Decreased body temperature
Infective endocarditis is often associated with fever, which would lead to an elevated body temperature rather than a decreased one.
Similar Questions
A nurse is creating a plan of care for a child who is awake and responsive following an acute head injury. Which of the following interventions should the nurse include?
A. Place the child in a room with bright fluorescent lighting.
Place the child in a room with bright fluorescent lighting.This option is not appropriate because bright fluorescent lighting can be uncomfortable and potentially aggravate symptoms such as headache or sensitivity to light, which are common after a head injury. Therefore, it is not included in the plan of care.
B. Initiate seizure precautions for the child.
Initiate seizure precautions for the child.This intervention is appropriate because children with head injuries are at an increased risk of seizures. Seizure precautions may include ensuring a safe environment, such as padding the sides of the bed, removing any objects that could cause harm during a seizure, and closely monitoring the child's neurological status for signs of seizure activity.
C. Use the COMFORT scale to rate the child's pain.
Use the COMFORT scale to rate the child's pain. While assessing and managing pain is important, the COMFORT scale may not be the most appropriate tool for evaluating pain in a child with a head injury. The nurse should use a pain assessment tool that is specifically designed for pediatric patients and is suitable for assessing pain in children with head injuries.
D. Suction the child's nares to determine the presence of fluid.
Suction the child's nares to determine the presence of fluid.Suctioning the child's nares may be indicated if there are concerns about airway patency or respiratory secretions. However, it is not a routine intervention for all children with head injuries. The nurse should assess the child's respiratory status and use suctioning only if necessary based on clinical findings.
Full Explanation
A. Place the child in a room with bright fluorescent lighting.
This option is not appropriate because bright fluorescent lighting can be uncomfortable and potentially aggravate symptoms such as headache or sensitivity to light, which are common after a head injury. Therefore, it is not included in the plan of care.
B. Initiate seizure precautions for the child.
This intervention is appropriate because children with head injuries are at an increased risk of seizures. Seizure precautions may include ensuring a safe environment, such as padding the sides of the bed, removing any objects that could cause harm during a seizure, and closely monitoring the child's neurological status for signs of seizure activity.
C. Use the COMFORT scale to rate the child's pain.
While assessing and managing pain is important, the COMFORT scale may not be the most appropriate tool for evaluating pain in a child with a head injury. The nurse should use a pain assessment tool that is specifically designed for pediatric patients and is suitable for assessing pain in children with head injuries.
D. Suction the child's nares to determine the presence of fluid.
Suctioning the child's nares may be indicated if there are concerns about airway patency or respiratory secretions. However, it is not a routine intervention for all children with head injuries. The nurse should assess the child's respiratory status and use suctioning only if necessary based on clinical findings.
A nurse is admitting a child who has bacterial meningitis. Which of the following actions should the nurse take first?
A. Initiate antibiotic therapy for the child.
Initiate antibiotic therapy for the child.This is the priority action. Bacterial meningitis is a medical emergency, and prompt administration of antibiotics is crucial to treat the infection and prevent further complications. Therefore, the nurse should initiate antibiotic therapy as soon as possible after obtaining appropriate cultures.
B. Minimize the child's environmental stimuli.
Minimize the child's environmental stimuli.While reducing environmental stimuli can help decrease the child's discomfort and prevent agitation, it is not the priority action when managing bacterial meningitis. Treating the underlying infection takes precedence to prevent serious complications such as neurological damage or septic shock.
C. Place the child in a side-lying position.
Place the child in a side-lying position. Positioning the child on their side may help prevent aspiration if vomiting occurs, but it is not the priority action in the initial management of bacterial meningitis. The child's positioning can be adjusted as needed once antibiotic therapy has been initiated.
D. Administer pain medication to the child.
Administer pain medication to the child.Pain management is important for the child's comfort, but it is not the priority action when managing bacterial meningitis. The child's pain may be addressed once antibiotic therapy has been initiated and the child's condition has stabilized.
Full Explanation
A. Initiate antibiotic therapy for the child.
This is the priority action. Bacterial meningitis is a medical emergency, and prompt administration of antibiotics is crucial to treat the infection and prevent further complications. Therefore, the nurse should initiate antibiotic therapy as soon as possible after obtaining appropriate cultures.
B. Minimize the child's environmental stimuli.
While reducing environmental stimuli can help decrease the child's discomfort and prevent agitation, it is not the priority action when managing bacterial meningitis. Treating the underlying infection takes precedence to prevent serious complications such as neurological damage or septic shock.
C. Place the child in a side-lying position.
Positioning the child on their side may help prevent aspiration if vomiting occurs, but it is not the priority action in the initial management of bacterial meningitis. The child's positioning can be adjusted as needed once antibiotic therapy has been initiated.
D. Administer pain medication to the child.
Pain management is important for the child's comfort, but it is not the priority action when managing bacterial meningitis. The child's pain may be addressed once antibiotic therapy has been initiated and the child's condition has stabilized.
A nurse is caring for a 4-month-old infant who is immediately postoperative following cleft palate repair. Which of the following actions should the nurse take?
A. Give the infant liquids using a small spoon with a long handle.
Give the infant liquids using a small spoon with a long handle.While feeding is essential, the method described is not specific to postoperative care after cleft palate repair.Feedings are resumed by bottle, breast/chest, or cup per surgeon preference; some surgeons prescribe the use of an Asepto syringe for feeding or a soft cup such as a soft-tipped sippy cup.
B. Apply elbow restraints to the infant.
Apply elbow restraints to the infant is correct.Elbow restraints would be used to prevent the infant from injuring or traumatizing the surgical site.
C. Gently check the infant's suture line using a padded tongue depressor.
Gently check the infant's suture line using a padded tongue depressor. It's important to assess the surgical site for signs of infection or bleeding, but using a padded tongue depressor may not be the most appropriate method. The nurse should follow the surgeon's orders regarding wound care and assessment techniques, which may include visual inspection without manipulation.
D. Place the infant in a supine position.
Place the infant in a supine position.Placing the infant in a supine position is generally recommended after cleft palate repair surgery to minimize strain on the surgical site and promote healing. However, it's essential to ensure proper positioning to prevent aspiration and maintain airway patency.
Full Explanation
A. Give the infant liquids using a small spoon with a long handle.
Give the infant liquids using a small spoon with a long handle.While feeding is essential, the method described is not specific to postoperative care after cleft palate repair.Feedings are resumed by bottle, breast/chest, or cup per surgeon preference; some surgeons prescribe the use of an Asepto syringe for feeding or a soft cup such as a soft-tipped sippy cup.
B. Apply elbow restraints to the infant.
Apply elbow restraints to the infant is correct.Elbow restraints would be used to prevent the infant from injuring or traumatizing the surgical site.
C. Gently check the infant's suture line using a padded tongue depressor.
It's important to assess the surgical site for signs of infection or bleeding, but using a padded tongue depressor may not be the most appropriate method. The nurse should follow the surgeon's orders regarding wound care and assessment techniques, which may include visual inspection without manipulation.
D. Place the infant in a supine position.
Placing the infant in a supine position is generally recommended after cleft palate repair surgery to minimize strain on the surgical site and promote healing. However, it's essential to ensure proper positioning to prevent aspiration and maintain airway patency.