Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is assisting with the care of a client who is in labor. The client's labor is difficult and prolonged and she reports a severe backache. Which of the following factors is a contributing cause of difficult, prolonged labor?
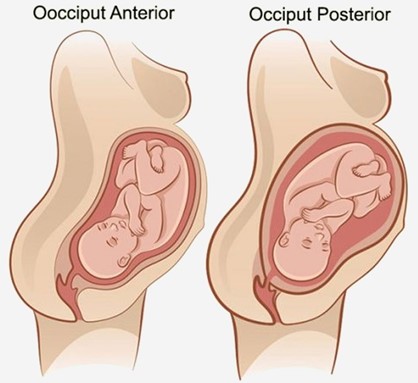
A. Fetal position is persistent occiput posterior.
Choice A reason: Fetal position is persistent occiput posterior is correct, as this position can cause difficult, prolonged labor and severe backache. The occiput posterior position means that the back of the fetal head is facing the maternal sacrum, which can result in poor alignment and descent, increased pressure on the maternal sacrum and nerves, and increased risk of perineal trauma. The nurse should encourage the client to change positions frequently, use pelvic rocking exercises, apply counterpressure to the sacrum, and administer analgesics as needed.
B. Fetal attitude is in general flexion.
Choice B reason: Fetal attitude is in general flexion is incorrect, as this attitude can facilitate normal labor and delivery. The fetal attitude refers to the degree of flexion or extension of the fetal head and limbs in relation to the fetal trunk. General flexion means that the fetal head is flexed on the chest, the arms are crossed over the chest, and the legs are flexed at the knees. This attitude allows the smallest diameter of the fetal head to pass through the birth canal.
C. Fetal lie is longitudinal.
Choice C reason: Fetal lie is longitudinal is incorrect, as this lie can facilitate normal labor and delivery. The fetal lie refers to the relationship between the long axis of the fetus and the long axis of the mother. Longitudinal lie means that both axes are parallel, which allows for either a vertex (head-first) or a breech (butocks-first) presentation.
D. Maternal pelvis is gynecoid.
Choice D reason: Maternal pelvis is gynecoid is incorrect, as this pelvis can facilitate normal labor and delivery. The maternal pelvis refers to the shape and size of the bony pelvis that affects the passage of the fetus. Gynecoid pelvis is the most common and favorable type for vaginal birth, as it has a rounded inlet, a wide pubic arch, and adequate outlet dimensions.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Proctored Exam. Take the full exam now
Full Explanation
Choice A reason:
Fetal position is persistent occiput posterior is correct, as this position can cause difficult, prolonged labor and severe backache. The occiput posterior position means that the back of the fetal head is facing the maternal sacrum, which can result in poor alignment and descent, increased pressure on the maternal sacrum and nerves, and increased risk of perineal trauma. The nurse should encourage the client to change positions frequently, use pelvic rocking exercises, apply counterpressure to the sacrum, and administer analgesics as needed.
Choice B reason:
Fetal attitude is in general flexion is incorrect, as this attitude can facilitate normal labor and delivery. The fetal attitude refers to the degree of flexion or extension of the fetal head and limbs in relation to the fetal trunk. General flexion means that the fetal head is flexed on the chest, the arms are crossed over the chest, and the legs are flexed at the knees. This attitude allows the smallest diameter of the fetal head to pass through the birth canal.
Choice C reason:
Fetal lie is longitudinal is incorrect, as this lie can facilitate normal labor and delivery. The fetal lie refers to the relationship between the long axis of the fetus and the long axis of the mother. Longitudinal lie means that both axes are parallel, which allows for either a vertex (head-first) or a breech (butocks-first) presentation.
Choice D reason:
Maternal pelvis is gynecoid is incorrect, as this pelvis can facilitate normal labor and delivery. The maternal pelvis refers to the shape and size of the bony pelvis that affects the passage of the fetus. Gynecoid pelvis is the most common and favorable type for vaginal birth, as it has a rounded inlet, a wide pubic arch, and adequate outlet dimensions.
Similar Questions
A nurse is assisting in the care of a client who is in the second stage of labor. Which of the following findings should the nurse report to the provider?
A. Bloody show from the vagina
Choice A reason: Bloody show from the vagina is incorrect, as this finding is normal and expected in the second stage of labor. Bloody show refers to the passage of mucus and blood from the cervix, which indicates cervical dilation and effacement.
B. Early decelerations in the FHR
Choice B reason: Early decelerations in the FHR is incorrect, as this finding is normal and benign in the second stage of labor. Early decelerations are symmetrical decreases in the FHR that mirror the contractions, which indicate fetal head compression and vagal stimulation. The nurse should continue to monitor the FHR and document the findings.
C. Pelvic pressure with contractions
Choice C reason: Pelvic pressure with contractions is incorrect, as this finding is normal and expected in the second stage of labor. Pelvic pressure indicates that the fetus is descending into the birth canal and that the client is ready to push.
D. Uterine contraction lasting 2 min
Choice D reason: Uterine contraction lasting 2 min is correct, as this finding is abnormal and potentially dangerous in any stage of labor. Uterine contraction lasting 2 min can indicate uterine tetany or hyperstimulation, which can cause fetal distress, placental abruption, uterine rupture, or maternal hemorrhage. The nurse should report this finding to the provider immediately and prepare to intervene as ordered.
Full Explanation
Choice A reason:
Bloody show from the vagina is incorrect, as this finding is normal and expected in the second stage of labor. Bloody show refers to the passage of mucus and blood from the cervix, which indicates cervical dilation and effacement.
Choice B reason:
Early decelerations in the FHR is incorrect, as this finding is normal and benign in the second stage of labor. Early decelerations are symmetrical decreases in the FHR that mirror the contractions, which indicate fetal head compression and vagal stimulation. The nurse should continue to monitor the FHR and document the findings.
Choice C reason:
Pelvic pressure with contractions is incorrect, as this finding is normal and expected in the second stage of labor. Pelvic pressure indicates that the fetus is descending into the birth canal and that the client is ready to push.
Choice D reason:
Uterine contraction lasting 2 min is correct, as this finding is abnormal and potentially dangerous in any stage of labor. Uterine contraction lasting 2 min can indicate uterine tetany or hyperstimulation, which can cause fetal distress, placental abruption, uterine rupture, or maternal hemorrhage. The nurse should report this finding to the provider immediately and prepare to intervene as ordered.

A nurse is preparing to administer dinoprostone gel to a client who is pregnant. The client asks the nurse about the purpose of the medication. Which of the following responses should the nurse make?
A. Dinoprostone stimulates uterine contractions.
Choice A reason: Dinoprostone stimulates uterine contractions is incorrect, as this is not the primary purpose of the medication. Dinoprostone is a prostaglandin that can induce labor by ripening the cervix and enhancing uterine contractility, but it is not used solely for stimulating contractions.
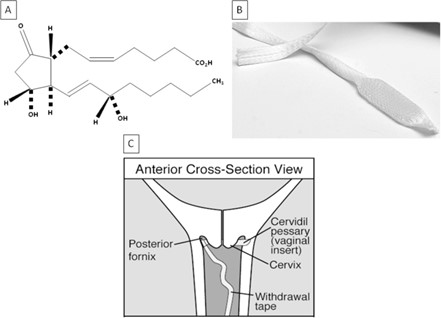
B. Dinoprostone promotes softening of the cervix.
Choice B reason: Dinoprostone promotes softening of the cervix is correct, as this is the main purpose of the medication. Dinoprostone is used to prepare the cervix for labor by increasing its softness, dilation, and effacement. This can facilitate the descent of the fetus and shorten the duration of labor.
C. Dinoprostone relaxes uterine contractions.
Choice C reason: Dinoprostone relaxes uterine contractions is incorrect, as this is the opposite effect of the medication. Dinoprostone can increase uterine tone and frequency, which can help initiate or augment labor. The nurse should monitor the client for signs of uterine hyperstimulation or fetal distress.
D. Dinoprostone assists with ending the pregnancy.
Choice D reason: Dinoprostone assists with ending the pregnancy is incorrect, as this is not the intended use of the medication. Dinoprostone can be used to terminate a pregnancy in some cases, such as fetal demise or missed abortion, but it is not routinely used for this purpose. The nurse should explain to the client that dinoprostone is used to induce labor and not to end a pregnancy.
Full Explanation
Choice A reason:
Dinoprostone stimulates uterine contractions is incorrect, as this is not the primary purpose of the medication. Dinoprostone is a prostaglandin that can induce labor by ripening the cervix and enhancing uterine contractility, but it is not used solely for stimulating contractions.
Choice B reason:
Dinoprostone promotes softening of the cervix is correct, as this is the main purpose of the medication. Dinoprostone is used to prepare the cervix for labor by increasing its softness, dilation, and effacement. This can facilitate the descent of the fetus and shorten the duration of labor.
Choice C reason:
Dinoprostone relaxes uterine contractions is incorrect, as this is the opposite effect of the medication. Dinoprostone can increase uterine tone and frequency, which can help initiate or augment labor. The nurse should monitor the client for signs of uterine hyperstimulation or fetal distress.
Choice D reason:
Dinoprostone assists with ending the pregnancy is incorrect, as this is not the intended use of the medication. Dinoprostone can be used to terminate a pregnancy in some cases, such as fetal demise or missed abortion, but it is not routinely used for this purpose. The nurse should explain to the client that dinoprostone is used to induce labor and not to end a pregnancy.
A nurse is assisting with the monitoring of a client who is in the first stage of labor, with an external fetal monitor in place and IV fluids infusing. Which of the following factors will cause variable decelerations in the fetal heart rate?
A. Maternal opioid administration
Choice A reason: Maternal opioid administration is incorrect, as this factor can cause late decelerations in the fetal heart rate. Late decelerations are symmetrical decreases in the FHR that begin after the peak of the contraction and return to baseline after the contraction ends, which indicate uteroplacental insufficiency. Maternal opioid administration can reduce maternal blood pressure and placental perfusion, leading to fetal hypoxia.
B. Fetal head compression
Choice B reason: Fetal head compression is incorrect, as this factor can cause early decelerations in the fetal heart rate. Early decelerations are symmetrical decreases in the FHR that mirror the contractions, which indicate fetal head compression and vagal stimulation. Fetal head compression occurs as the fetus descends into the birth canal and does not pose a threat to the fetal well-being.
C. Uteroplacental insufficiency
Choice C reason: Uteroplacental insufficiency is incorrect, as this factor can cause late decelerations in the fetal heart rate. Uteroplacental insufficiency refers to a reduced blood flow and oxygen delivery to the fetus through the placenta, which can result from maternal hypotension, uterine hyperstimulation, placental abruption, or other conditions. Uteroplacental insufficiency can cause fetal hypoxia and acidosis.
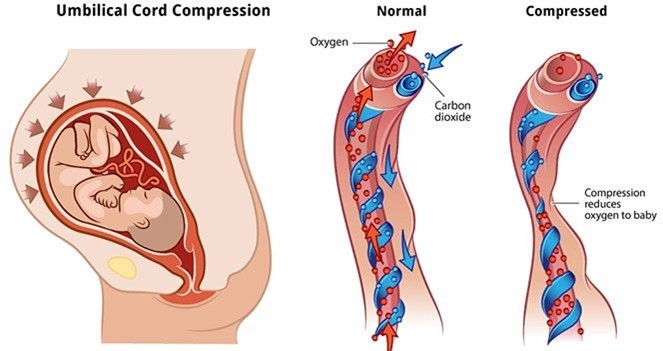
D. Umbilical cord compression
Choice D reason: Umbilical cord compression is correct, as this factor can cause variable decelerations in the fetal heart rate. Variable decelerations are abrupt decreases in the FHR that vary in onset, duration, and depth, which indicate umbilical cord compression and reduced blood flow to the fetus. Umbilical cord compression can occur due to cord prolapse, nuchal cord, short cord, or other causes. The nurse should reposition the client, administer oxygen, and prepare for delivery if indicated.
Full Explanation
Choice A reason:
Maternal opioid administration is incorrect, as this factor can cause late decelerations in the fetal heart rate. Late decelerations are symmetrical decreases in the FHR that begin after the peak of the contraction and return to baseline after the contraction ends, which indicate uteroplacental insufficiency. Maternal opioid administration can reduce maternal blood pressure and placental perfusion, leading to fetal hypoxia.
Choice B reason:
Fetal head compression is incorrect, as this factor can cause early decelerations in the fetal heart rate. Early decelerations are symmetrical decreases in the FHR that mirror the contractions, which indicate fetal head compression and vagal stimulation. Fetal head compression occurs as the fetus descends into the birth canal and does not pose a threat to the fetal well-being.
Choice C reason:
Uteroplacental insufficiency is incorrect, as this factor can cause late decelerations in the fetal heart rate. Uteroplacental insufficiency refers to a reduced blood flow and oxygen delivery to the fetus through the placenta, which can result from maternal hypotension, uterine hyperstimulation, placental abruption, or other conditions. Uteroplacental insufficiency can cause fetal hypoxia and acidosis.
Choice D reason:
Umbilical cord compression is correct, as this factor can cause variable decelerations in the fetal heart rate. Variable decelerations are abrupt decreases in the FHR that vary in onset, duration, and depth, which indicate umbilical cord compression and reduced blood flow to the fetus. Umbilical cord compression can occur due to cord prolapse, nuchal cord, short cord, or other causes. The nurse should reposition the client, administer oxygen, and prepare for delivery if indicated.