Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
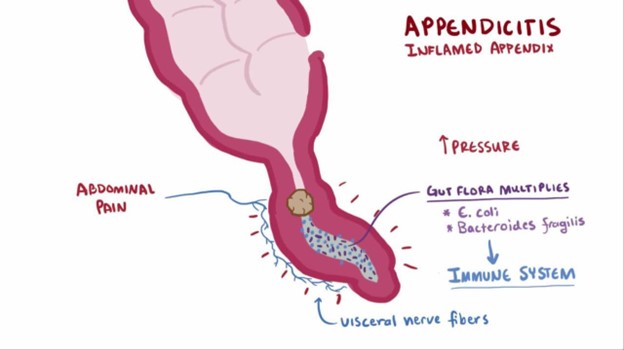
A nurse is caring for a child who has suspected appendicitis. Which of the following provider prescriptions should the nurse clarify?
A. Monitor oral temperature every 4 hr.
Monitoring oral temperature every 4 hours is important to assess for signs of infection or worsening condition.
B. Administer sodium biphosphate/sodium phosphate.
The nurse should clarify the prescription to administer sodium biphosphate/sodium phosphate because it is a laxative and is contraindicated in a child with suspected appendicitis. The use of laxatives or enemas can potentially worsen the condition by increasing the risk of perforation or rupture of the inflamed appendix.
C. Maintain NPO status.
Maintaining NPO status is essential to avoid stimulating the digestive system and to prepare for possible surgery.
D. Medicate the client for pain every 4 hr as needed.
Medicating the client for pain every 4 hours as needed is appropriate to manage pain and provide comfort while the child awaits further evaluation or treatment.Remember, it's crucial to avoid the use of laxatives, enemas, or any other interventions that can potentially aggravate the inflamed appendix in a child with suspected appendicitis.
This question is an excerpt from Nurse Dive's nursing test bank - SIMMONS U BSN PEDIATRICS PROCTORED EXAM. Take the full exam now
Full Explanation
The nurse should clarify the prescription to administer sodium biphosphate/sodium phosphate because it is a laxative and is contraindicated in a child with suspected appendicitis. The use of laxatives or enemas can potentially worsen the condition by increasing the risk of perforation or rupture of the inflamed appendix.
A. Monitoring oral temperature every 4 hours is important to assess for signs of infection or worsening condition.
C. Maintaining NPO status is essential to avoid stimulating the digestive system and to prepare for possible surgery.
D. Medicating the client for pain every 4 hours as needed is appropriate to manage pain and provide comfort while the child awaits further evaluation or treatment.
Remember, it's crucial to avoid the use of laxatives, enemas, or any other interventions that can potentially aggravate the inflamed appendix in a child with suspected appendicitis.
Similar Questions
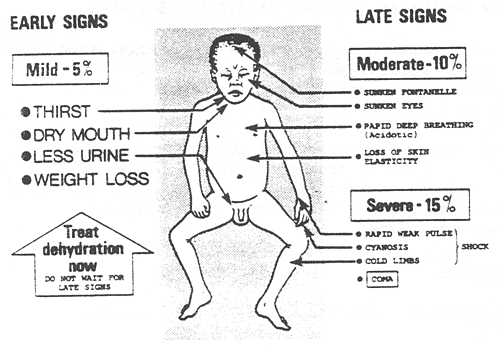
A nurse in an emergency department is assessing an infant who is dehydrated. Which of the following findings should the nurse expect?
A. Irritability
The nurse should expect to find irritability in an infant who is dehydrated. Dehydration in infants can lead to changes in behavior and irritability due to the imbalance in fluid and electrolytes. Other common signs of dehydration in infants may include: Poor skin turgor (skin tenting) Sunken fontanelles (soft spots on the baby's head) Dry mucous membranes (dry mouth and tongue) Decreased urine output or concentrated urine Rapid heart rate (tachycardia) Increased respiratory rate Sunken eyes Decreased tears when crying
B. Tetany
Tetany is a condition characterized by involuntary muscle contractions and is more commonly associated with hypocalcemia (low calcium levels) rather than dehydration.
C. slow, bounding pulse
A slow, bounding pulse is not typically associated with dehydration. Dehydration often leads to a rapid heart rate (tachycardia) as the body attempts to compensate for the loss of fluid.
D. Decreased temperature
Decreased temperature is not a typical finding in dehydration. Dehydration can lead to fever in some cases due to an underlying infection, but it does not cause a decrease in body temperature on its own.
Full Explanation
The nurse should expect to find irritability in an infant who is dehydrated. Dehydration in infants can lead to changes in behavior and irritability due to the imbalance in fluid and electrolytes. Other common signs of dehydration in infants may include:
Poor skin turgor (skin tenting)
Sunken fontanelles (soft spots on the baby's head)
Dry mucous membranes (dry mouth and tongue)
Decreased urine output or concentrated urine
Rapid heart rate (tachycardia)
Increased respiratory rate
Sunken eyes
Decreased tears when crying
B. Tetany is a condition characterized by involuntary muscle contractions and is more commonly associated with hypocalcemia (low calcium levels) rather than dehydration.
C. A slow, bounding pulse is not typically associated with dehydration. Dehydration often leads to a rapid heart rate (tachycardia) as the body attempts to compensate for the loss of fluid.
D. Decreased temperature is not a typical finding in dehydration. Dehydration can lead to fever in some cases due to an underlying infection, but it does not cause a decrease in body temperature on its own.
A nurse in an emergency department is caring for an infant who has a 2-day history of vomiting and an elevated temperature. Which of the following should the nurse recognize as the most reliable indicator of fluid loss?
A. Skin integrity
Option A: Skin integrity is important to assess for signs of dehydration, but it is not as reliable as body weight in determining the extent of fluid loss.
B. Respiratory rate
Option B: Respiratory rate can be affected by various factors and is not a direct indicator of fluid loss.
C. Body weight
In an infant with a history of vomiting and fever, body weight is the most reliable indicator of fluid loss. Monitoring the infant's weight over time can help assess the degree of dehydration and guide the appropriate fluid replacement therapy. A significant decrease in body weight suggests significant fluid loss.
D. Blood pressure
Option D: Blood pressure is not the most reliable indicator of fluid loss in an infant with dehydration. In severe cases of dehydration, blood pressure can drop, but it is not as sensitive as body weight in assessing the extent of fluid loss.
Full Explanation
In an infant with a history of vomiting and fever, body weight is the most reliable indicator of fluid loss. Monitoring the infant's weight over time can help assess the degree of dehydration and guide the appropriate fluid replacement therapy. A significant decrease in body weight suggests significant fluid loss.
Option A: Skin integrity is important to assess for signs of dehydration, but it is not as reliable as body weight in determining the extent of fluid loss.
Option B: Respiratory rate can be affected by various factors and is not a direct indicator of fluid loss.
Option D: Blood pressure is not the most reliable indicator of fluid loss in an infant with dehydration. In severe cases of dehydration, blood pressure can drop, but it is not as sensitive as body weight in assessing the extent of fluid loss.
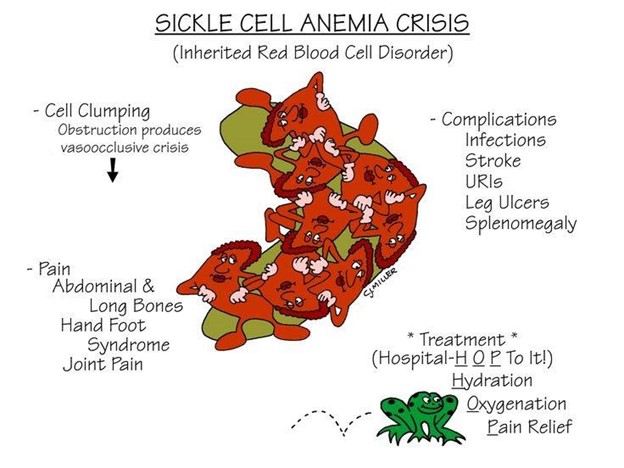
A nurse is assessing a child who is in a sickle cell crisis. Which of the following findings should the nurse expect?
A. Constipation
Constipation is not a common symptom of sickle cell crisis. It may be associated with other conditions but is not directly related to sickle cell crisis.
B. Pain
During a sickle cell crisis, the child experiences severe pain due to the sickled red blood cells blocking blood flow in the vessels, leading to tissue ischemia and infarction. Pain is the hallmark symptom of sickle cell crisis and can occur in various parts of the body, such as the abdomen, chest, back, joints, and extremities.
C. High fever
High fever is not a typical finding in sickle cell crisis. Fever may occur due to infections, which individuals with sickle cell disease are at increased risk of developing, but it is not a direct symptom of the crisis itself.
D. Bradycardia
Bradycardia (slow heart rate) is not commonly associated with sickle cell crisis. Tachycardia (rapid heart rate) may occur in response to pain, but bradycardia is not a typical finding.
Full Explanation
During a sickle cell crisis, the child experiences severe pain due to the sickled red blood cells blocking blood flow in the vessels, leading to tissue ischemia and infarction. Pain is the hallmark symptom of sickle cell crisis and can occur in various parts of the body, such as the abdomen, chest, back, joints, and extremities.
A. Constipation is not a common symptom of sickle cell crisis. It may be associated with other conditions but is not directly related to sickle cell crisis.
C. High fever is not a typical finding in sickle cell crisis. Fever may occur due to infections, which individuals with sickle cell disease are at increased risk of developing, but it is not a direct symptom of the crisis itself.
D. Bradycardia (slow heart rate) is not commonly associated with sickle cell crisis. Tachycardia (rapid heart rate) may occur in response to pain, but bradycardia is not a typical finding.