Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has chronic kidney disease (CKD) and states she has heartburn.
The provider prescribes aluminum hydroxide. The client asks, "Why can't I just take the antacid magaldrate my husband has at home?" The nurse explains to the client that aluminum hydroxide is the preferred antacid because it lowers which of the following?
A. Serum magnesium levels
Aluminum hydroxide can lead to increased serum magnesium levels, but this is not the reason for its preference in chronic kidney disease.
B. Serum phosphorus levels
Aluminum hydroxide is preferred because it binds to dietary phosphate, reducing serum phosphorus levels in patients with chronic kidney disease who are prone to hyperphosphatemia.
C. Serum potassium levels
Aluminum hydroxide does not significantly affect serum potassium levels.
D. Serum calcium levels
Aluminum hydroxide can lead to decreased serum calcium levels due to binding, but this is not the primary reason for its preference in chronic kidney disease.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Med Surg Proctored Exam 8. Take the full exam now
Full Explanation
A. Aluminum hydroxide can lead to increased serum magnesium levels, but this is not the reason for its preference in chronic kidney disease.
B. Aluminum hydroxide is preferred because it binds to dietary phosphate, reducing serum phosphorus levels in patients with chronic kidney disease who are prone to hyperphosphatemia.
C. Aluminum hydroxide does not significantly affect serum potassium levels.
D. Aluminum hydroxide can lead to decreased serum calcium levels due to binding, but this is not the primary reason for its preference in chronic kidney disease.
Similar Questions
A nurse is reviewing the arterial blood gas results for a client in the ICU who has kidney failure and determines the client has respiratory acidosis. Which of the following findings should the nurse expect?
A. Warm flushed skin
Respiratory acidosis typically presents with cool, clammy skin due to compensatory peripheral vasoconstriction.
B. Bounding peripheral pulses
Peripheral pulses may be weak or thready in respiratory acidosis due to decreased cardiac output.
C. Widened QRS complexes
Respiratory acidosis can lead to electrolyte imbalances, particularly hyperkalemia, which can manifest as widened QRS complexes on an electrocardiogram (ECG).
D. Hyperactive deep tendon reflexes
Respiratory acidosis can lead to hyperkalemia, but hyperactive deep tendon reflexes are not a characteristic finding.
Full Explanation
A. Respiratory acidosis typically presents with cool, clammy skin due to compensatory peripheral vasoconstriction.
B. Peripheral pulses may be weak or thready in respiratory acidosis due to decreased cardiac output.
C. Respiratory acidosis can lead to electrolyte imbalances, particularly hyperkalemia, which can manifest as widened QRS complexes on an electrocardiogram (ECG).
D. Respiratory acidosis can lead to hyperkalemia, but hyperactive deep tendon reflexes are not a characteristic finding.
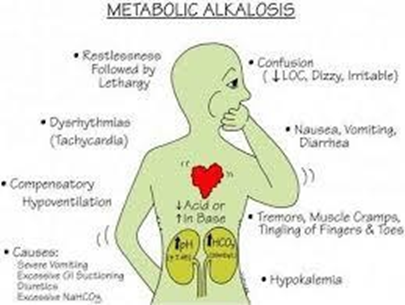
A nurse is caring for a client who has metabolic alkalosis. For which of the following clinical manifestations should the nurse monitor? (Select all that apply.)
A. Bicarbonate excess
Bicarbonate excess is not a clinical manifestation but rather the underlying cause of metabolic alkalosis.
B. Muscle weakness
Metabolic alkalosis can lead to potassium depletion, which may cause muscle weakness.
C. Kussmaul's respirations
Kussmaul's respirations, characterized by deep and labored breathing, are more commonly associated with metabolic acidosis, not alkalosis, as the body tries to compensate for acidemia by expelling more carbon dioxide through deep breaths.
D. Circumoral paresthesia
Alkalosis can cause peripheral vasodilation and decreased calcium ionization, leading to circumoral and digital paresthesia.
E. Dizziness
Alkalosis can cause cerebral vasoconstriction and decreased cerebral perfusion, leading to dizziness.
Full Explanation
A. Bicarbonate excess is not a clinical manifestation but rather the underlying cause of metabolic alkalosis.
B. Metabolic alkalosis can lead to potassium depletion, which may cause muscle weakness.
C. Kussmaul's respirations, characterized by deep and labored breathing, are more commonly associated with metabolic acidosis, not alkalosis, as the body tries to compensate for acidemia by expelling more carbon dioxide through deep breaths.
D. Alkalosis can cause peripheral vasodilation and decreased calcium ionization, leading to circumoral and digital paresthesia.
E. Alkalosis can cause cerebral vasoconstriction and decreased cerebral perfusion, leading to dizziness.
A nurse is assessing a client who is 2 weeks postoperative following a kidney transplant. Which of the following manifestations should the nurse identify as possible organ rejection?
A. Weight loss
Weight loss is not typically a manifestation of organ rejection post kidney transplant.
B. Insomnia
Insomnia is not typically associated with organ rejection post kidney transplant.
C. Temperature 36.1°C (97.0° F)
Normal body temperature does not indicate organ rejection post kidney transplant.
D. Oliguria
Oliguria or decreased urine output can be a sign of organ rejection post kidney transplant due to decreased renal perfusion.
Full Explanation
A. Weight loss is not typically a manifestation of organ rejection post kidney transplant.
B. Insomnia is not typically associated with organ rejection post kidney transplant.
C. Normal body temperature does not indicate organ rejection post kidney transplant.
D. Oliguria or decreased urine output can be a sign of organ rejection post kidney transplant due to decreased renal perfusion.