Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has Cushing’s syndrome. Which of the following clinical manifestations should the nurse expect to observe? (Select all that apply.)
A. Purple striations
Choice A: Purple striations. These are also known as striae, and they are caused by the thinning and weakening of the skin and underlying connective tissue due to cortisol. They appear as purple or red lines on the abdomen, thighs, breasts, or arms.
B. Tremors
Choice B: Tremors. These are not a clinical manifestation of Cushing’s syndrome, but rather a sign of hyperthyroidism, which is a condition caused by excess thyroid hormone production or exposure. Thyroid hormone affects the nervous system and causes increased muscle activity and tremors.
C. Buffalo hump
Choice C: Buffalo hump. This is a term used to describe the accumulation of fat on the upper back and neck due to cortisol. It gives the appearance of a hump or a rounded shape.
D. Obese extremities
Choice D: Obese extremities. These are not a clinical manifestation of Cushing’s syndrome, but rather a sign of hypothyroidism, which is a condition caused by low thyroid hormone production or exposure. Thyroid hormone affects the metabolism of carbohydrates, proteins, and fats, and causes decreased energy expenditure and weight gain.
E. Moon face
Choice E: Moon face. This is a term used to describe the rounding and fullness of the face due to cortisol. It gives the appearance of a moon-like shape.
This question is an excerpt from Nurse Dive's nursing test bank - ATI LPN Med Surg Proctored Exam. Take the full exam now
Full Explanation
Choice A: Purple striations. These are also known as striae, and they are caused by the thinning and weakening of the skin and underlying connective tissue due to cortisol. They appear as purple or red lines on the abdomen, thighs, breasts, or arms.
Choice C: Buffalo hump. This is a term used to describe the accumulation of fat on the upper back and neck due to cortisol. It gives the appearance of a hump or a rounded shape.
Choice E: Moon face. This is a term used to describe the rounding and fullness of the face due to cortisol. It gives the
appearance of a moon-like shape.
Choice B: Tremors. These are not a clinical manifestation of Cushing’s syndrome, but rather a sign of hyperthyroidism, which is a condition caused by excess thyroid hormone production or exposure. Thyroid hormone affects the nervous system and causes increased muscle activity and tremors.
Choice D: Obese extremities. These are not a clinical manifestation of Cushing’s syndrome, but rather a sign of hypothyroidism, which is a condition caused by low thyroid hormone production or exposure. Thyroid hormone affects the metabolism of carbohydrates, proteins, and fats, and causes decreased energy expenditure and weight gain.
Similar Questions
A nurse is collecting data from a client who has diverticular disease. The nurse should expect the client to report abdominal pain in which of the following locations?
A. Upper left quadrant
Choice A: Upper left quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The upper left quadrant of the abdomen contains organs such as the stomach, spleen, pancreas, and part of the colon. Abdominal pain in this area can indicate conditions such as gastritis, peptic ulcer, pancreatitis, splenomegaly, or colon cancer.
B. Lower left quadrant
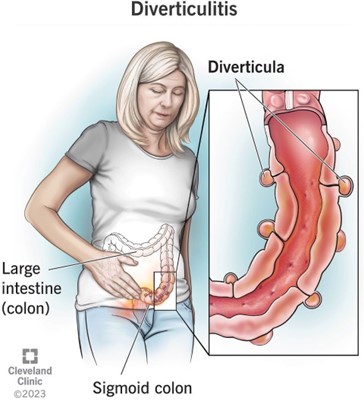
Choice B: Lower left quadrant. This is the location where the nurse should expect the client to report abdominal pain who has diverticular disease, which is a condition that involves the formation of pouches or sacs in the wall of the colon. These pouches or sacs are called diverticula, and they can become inflamed or infected, causing diverticulitis. Diverticulitis can cause abdominal pain, fever, nausea, vomiting, and changes in bowel habits. The most common site of diverticula formation and diverticulitis is the sigmoid colon, which is located in the lower left quadrant of the abdomen.
C. Upper right quadrant
Choice C: Upper right quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The upper right quadrant of the abdomen contains organs such as the liver, gallbladder, duodenum, and part of the colon. Abdominal pain in this area can indicate conditions such as hepatitis, cholecystitis, duodenal ulcer, or colon cancer.
D. Lower right quadrant
Choice D: Lower right quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The lower right quadrant of the abdomen contains organs such as the appendix, cecum, and part of the colon. Abdominal pain in this area can indicate conditions such as appendicitis, Crohn’s disease, or colon cancer.
Full Explanation
Choice A: Upper left quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The upper left quadrant of the abdomen contains organs such as the stomach, spleen, pancreas, and part of the colon. Abdominal pain in this area can indicate conditions such as gastritis, peptic ulcer, pancreatitis, splenomegaly, or colon cancer.
Choice B: Lower left quadrant. This is the location where the nurse should expect the client to report abdominal pain who has diverticular disease, which is a condition that involves the formation of pouches or sacs in the wall of the colon. These pouches or sacs are called diverticula, and they can become inflamed or infected, causing diverticulitis. Diverticulitis can cause abdominal pain, fever, nausea, vomiting, and changes in bowel habits. The most common site of diverticula formation and diverticulitis is the sigmoid colon, which is located in the lower left quadrant of the abdomen.
Choice C: Upper right quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The upper right quadrant of the abdomen contains organs such as the liver, gallbladder, duodenum, and part of the colon. Abdominal pain in this area can indicate conditions such as hepatitis, cholecystitis, duodenal ulcer, or colon cancer.
Choice D: Lower right quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The lower right quadrant of the abdomen contains organs such as the appendix, cecum, and part of the colon. Abdominal pain in this area can indicate conditions such as appendicitis, Crohn’s disease, or colon cancer.
A nurse is assisting with the plan of care for a client who has hypothyroidism with myxedema. Which of the following interventions should the nurse include in the plan of care?
A. Place the client on bedrest.
Choice A: Place the client on bedrest. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Placing the client on bedrest can increase the risk of complications such as thromboembolism, pressure ulcers, and muscle atrophy. The nurse should encourage the client to perform gentle exercises and change positions frequently.
B. Apply warm blankets.
Choice B: Apply warm blankets. This is an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Hypothyroidism is a condition that occurs when the thyroid gland does not produce enough thyroid hormone. Thyroid hormone regulates the metabolism of carbohydrates, proteins, and fats, and affects the energy expenditure and body temperature. Myxedema is a severe form of hypothyroidism that causes swelling of the skin and tissues due to accumulation of mucopolysaccharides. Applying warm blankets can help maintain the client’s body temperature and prevent hypothermia, which is a low body temperature.
C. Check the client for weight loss.
Choice C: Check the client for weight loss. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Checking the client for weight loss can indicate hyperthyroidism, which is a condition that occurs when the thyroid gland produces too much thyroid hormone. Hyperthyroidism can cause weight loss due to increased metabolic rate and appetite. The nurse should check the client for weight gain, which can indicate hypothyroidism due to decreased metabolic rate and fluid retention.
D. Limit high-fiber foods.
Choice D: Limit high-fiber foods. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Limiting high-fiber foods can cause constipation, which can worsen hypothyroidism symptoms such as bloating, abdominal pain, and fatigue. The nurse should encourage the client to eat high-fiber foods, such as fruits, vegetables, and whole grains, to promote bowel regularity and prevent constipation.
Full Explanation
Choice A: Place the client on bedrest. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Placing the client on bedrest can increase the risk of complications such as thromboembolism, pressure ulcers, and muscle atrophy. The nurse should encourage the client to perform gentle exercises and change positions frequently.
Choice B: Apply warm blankets. This is an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Hypothyroidism is a condition that occurs when the thyroid gland does not produce enough thyroid hormone. Thyroid hormone regulates the metabolism of carbohydrates, proteins, and fats, and affects the energy expenditure and body temperature. Myxedema is a severe form of hypothyroidism that causes swelling of the skin and tissues due to accumulation of mucopolysaccharides. Applying warm blankets can help maintain the client’s body temperature and prevent hypothermia, which is a low body temperature.
Choice C: Check the client for weight loss. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Checking the client for weight loss can indicate hyperthyroidism, which is a condition that occurs when the thyroid gland produces too much thyroid hormone.
Hyperthyroidism can cause weight loss due to increased metabolic rate and appetite. The nurse should check the client for weight gain, which can indicate hypothyroidism due to decreased metabolic rate and fluid retention.
Choice D: Limit high-fiber foods. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Limiting high-fiber foods can cause constipation, which can worsen hypothyroidism symptoms such as bloating, abdominal pain, and fatigue. The nurse should encourage the client to eat high-fiber foods, such as fruits, vegetables, and whole grains, to promote bowel regularity and prevent constipation.
A nurse is contributing to the plan of care for a client who has cirrhosis and ascites. Which of the following interventions should the nurse recommend for inclusion in the plan of care?
A. Increase the client’s sodium intake.
Choice A: Increase the client’s sodium intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Increasing the client’s sodium intake can worsen fluid retention and exacerbate ascites. The nurse should recommend limiting the client’s sodium intake to less than 2 g per day.
B. Decrease the client’s fluid intake.
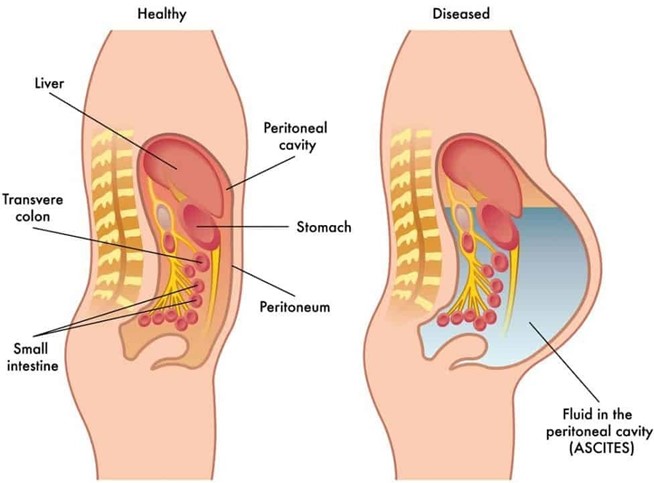
Choice B: Decrease the client’s fluid intake. This is an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Cirrhosis is a chronic liver disease that causes scarring and impaired liver function. Ascites is a complication of cirrhosis that involves accumulation of fluid in the peritoneal cavity. Decreasing the client’s fluid intake can help reduce fluid retention and prevent further distension of the abdomen and pressure on the diaphragm.
C. Increase the client’s saturated fat intake.
Choice C: Increase the client’s saturated fat intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Increasing the client’s saturated fat intake can increase the risk of cardiovascular disease, obesity, and faty liver disease. The nurse should recommend a balanced diet that provides adequate protein, calories, vitamins, and minerals.
D. Decrease the client’s carbohydrate intake
Choice D: Decrease the client’s carbohydrate intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Decreasing the client’s carbohydrate intake can cause ketosis, which is a metabolic state that occurs when the body uses fat as a fuel source instead of glucose. Ketosis can cause nausea, fatigue, headache, and bad breath. The nurse should recommend a moderate carbohydrate intake that provides enough glucose for energy and prevents ketosis.
Full Explanation
Choice A: Increase the client’s sodium intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Increasing the client’s sodium intake can worsen fluid retention and exacerbate ascites. The nurse should recommend limiting the client’s sodium intake to less than 2 g per day.
Choice B: Decrease the client’s fluid intake. This is an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Cirrhosis is a chronic liver disease that causes scarring and impaired liver function. Ascites is a complication of cirrhosis that involves the accumulation of fluid in the peritoneal cavity. Decreasing the client’s fluid intake can help reduce fluid retention and prevent further distension of the abdomen and pressure on the diaphragm.
Choice C: Increase the client’s saturated fat intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Increasing the client’s saturated fat intake can increase the risk of cardiovascular disease, obesity, and faty liver disease. The nurse should recommend a balanced diet that provides adequate protein, calories, vitamins, and minerals.
Choice D: Decrease the client’s carbohydrate intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Decreasing the client’s carbohydrate intake can cause ketosis, which is a metabolic state that occurs when the body uses fat as a fuel source instead of glucose.
Ketosis can cause nausea, fatigue, headache, and bad breath. The nurse should recommend a moderate carbohydrate intake that provides enough glucose for energy and prevents ketosis.