Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has developed a Clostridium difficile infection following antibiotic therapy. Which of the following actions should the nurse take?
A. Implement neutropenia isolation.
Choice A: Implement neutropenia isolation. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Neutropenia isolation is a type of protective isolation that is used for clients who have low white blood cell counts and are at risk of infection from others. It is not indicated for clients who have Clostridium difficile infection, which is not transmited through the air.
B. Use alcohol hand sanitizer following client care.
Choice B: Use alcohol hand sanitizer following client care. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Alcohol hand sanitizer is ineffective against Clostridium difficile spores and can increase the risk of transmission. The nurse should wash their hands with soap and water, which can remove the spores from the skin.
C. Monitor the client for manifestations of fluid overload.
Choice C: Monitor the client for manifestations of fluid overload. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Fluid overload is a condition that occurs when the body retains excess fluid and causes symptoms such as edema, dyspnea, and hypertension. It is not related to Clostridium difficile infection, which can cause fluid loss due to diarrhea and dehydration. The nurse should monitor the client for manifestations of fluid deficit, such as dry mucous membranes, tachycardia, and hypotension.
D. Disinfect equipment with bleach solution
Choice D: Disinfect equipment with bleach solution. This is an action that the nurse should take for a client who has developed a Clostridium difficile infection, which is a bacterial infection that causes severe diarrhea and inflammation of the colon. Clostridium difficile spores are resistant to most disinfectants and can survive on surfaces for a long time. The nurse should disinfect equipment with bleach solution, which can kill the spores and prevent transmission.
This question is an excerpt from Nurse Dive's nursing test bank - ATI LPN Med Surg Proctored Exam. Take the full exam now
Full Explanation
Choice A: Implement neutropenia isolation. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Neutropenia isolation is a type of protective isolation that is used for
clients who have low white blood cell counts and are at risk of infection from others. It is not indicated for clients who have Clostridium difficile infection, which is not transmited through the air.
Choice B: Use alcohol hand sanitizer following client care. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Alcohol hand sanitizer is ineffective against Clostridium difficile spores and can increase the risk of transmission. The nurse should wash their hands with soap and water, which can remove the spores from the skin.
Choice C: Monitor the client for manifestations of fluid overload. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Fluid overload is a condition that occurs when the body retains excess fluid and causes symptoms such as edema, dyspnea, and hypertension. It is not related to Clostridium difficile infection, which can cause fluid loss due to diarrhea and dehydration. The nurse should monitor the client for manifestations of fluid deficit, such as dry mucous membranes, tachycardia, and hypotension.
Choice D: Disinfect equipment with bleach solution. This is an action that the nurse should take for a client who has developed a Clostridium difficile infection, which is a bacterial infection that causes severe diarrhea and inflammation of the colon. Clostridium difficile spores are resistant to most disinfectants and can survive on surfaces for a long time. The nurse should disinfect equipment with bleach solution, which can kill the spores and prevent transmission.
Similar Questions
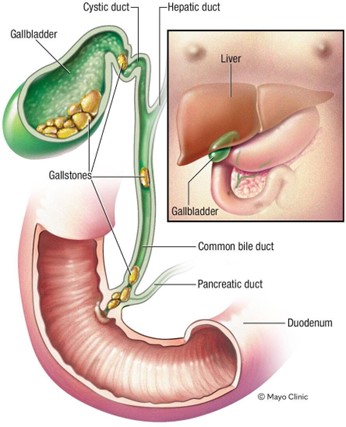
A nurse is collecting data from a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Which of the following findings is expected for this condition?
A. Faty stools
Choice A: Faty stools. This is a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis, which is the presence of gallstones in the gallbladder or bile ducts. The common bile duct carries bile from the liver and gallbladder to the duodenum, where it helps digest fats. If the common bile duct is obstructed by a gallstone, bile cannot reach the duodenum and fats cannot be properly absorbed. This results in fatty stools, which are also known as steatorrhea. Fatty stools are pale, bulky, greasy, and foul-smelling.
B. Ecchymosis of the extremities
Choice B: Ecchymosis of the extremities. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Ecchymosis of the extremities is a sign of bleeding under the skin, which can be caused by trauma, coagulation disorders, or medications. It is not related to bile duct obstruction or gallstones.
C. Straw-colored urine
Choice C: Straw-colored urine. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Straw-coloured urine is a normal colour of urine, which indicates adequate hydration and kidney function. It is not affected by bile duct obstruction or gallstones.
D. Tenderness in the left upper abdomen
Choice D: Tenderness in the left upper abdomen. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Tenderness in the left upper abdomen is a sign of splenomegaly, which is an enlargement of the spleen due to infection, inflammation, or cancer. It is not related to bile duct obstruction or gallstones.
Full Explanation
Choice A: Faty stools. This is a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis, which is the presence of gallstones in the gallbladder or bile ducts. The common bile duct carries bile from the liver and gallbladder to the duodenum, where it helps digest fats. If the common bile duct is obstructed by a gallstone, bile cannot reach the duodenum and fats cannot be properly absorbed. This results in fatty stools, which are also known as steatorrhea. Fatty stools are pale, bulky, greasy, and foul-smelling.
Choice B: Ecchymosis of the extremities. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Ecchymosis of the extremities is a sign of bleeding under the skin, which can be caused by trauma, coagulation disorders, or medications. It is not related to bile duct obstruction or gallstones.
Choice C: Straw-colored urine. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Straw-coloured urine is a normal colour of urine, which indicates adequate hydration and kidney function. It is not affected by bile duct obstruction or gallstones.
Choice D: Tenderness in the left upper abdomen. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Tenderness in the left upper abdomen is a sign of splenomegaly, which is an enlargement of the spleen due to infection, inflammation, or cancer. It is not related to bile duct obstruction or gallstones.
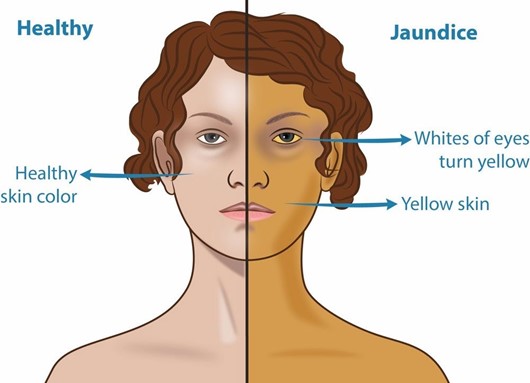
A nurse is collecting data from a client who is African American and has cholecystitis. Which of the following areas should the nurse inspect to monitor for the presence of jaundice?
A. Peri-umbilical area
Choice A: Peri-umbilical area. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The peri-umbilical area is the area around the navel, which is part of the skin. The skin can show jaundice, but it may be difficult to detect in clients with dark skin tones.
B. Nail beds
Choice B: Nail beds. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The nail beds are part of the skin that can show jaundice, but they may also be affected by other factors such as anemia, cyanosis, or nail polish.
C. Webbed areas of the fingers
Choice C: Webbed areas of the fingers. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The webbed areas of the fingers are part of the skin that can show jaundice, but they may also be influenced by other factors such as temperature, circulation, or pressure.
D. Hard palate
Choice D: Hard palate. This is an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis, which is an inflammation of the gallbladder. Jaundice is a yellowish discoloration of the skin and mucous membranes due to elevated bilirubin levels in the blood. Bilirubin is a pigment that is produced from the breakdown of red blood cells and is normally excreted in bile. If the gallbladder or bile ducts are inflamed or obstructed, bile cannot flow into the duodenum and bilirubin accumulates in the blood and tissues. The hard palate is a part of the oral mucosa that can show jaundice, especially in clients with dark skin tones.
Full Explanation
Choice A: Peri-umbilical area. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The peri-umbilical area is the area around the navel, which is part of the skin. The skin can show jaundice, but it may be difficult to detect in clients with dark skin tones.
Choice B: Nail beds. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The nail beds are part of the skin that can show jaundice, but they may also be affected by other factors such as anemia, cyanosis, or nail polish.
Choice C: Webbed areas of the fingers. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The webbed areas of the fingers are part of the skin that can show jaundice, but they may also be influenced by other factors such as temperature, circulation, or pressure.
Choice D: Hard palate. This is an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis, which is an inflammation of the gallbladder. Jaundice is a yellowish discoloration of the skin and mucous membranes due to elevated bilirubin levels in the blood. Bilirubin is a pigment that is produced from the breakdown of red blood cells and is normally excreted in bile. If the gallbladder or bile ducts are inflamed or obstructed, bile cannot flow into the duodenum and bilirubin accumulates in the blood and tissues. The hard palate is a part of the oral mucosa that can show jaundice, especially in clients with dark skin tones.
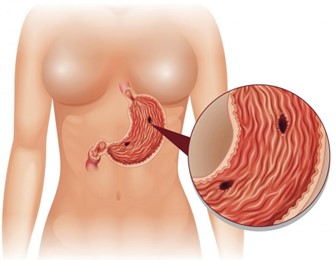
A nurse is collecting data from a client who has peptic ulcer disease. Which of the following findings is a manifestation of gastrointestinal perforation?
A. Bradycardia
Choice A: Bradycardia. This is not a manifestation of gastrointestinal perforation, but rather a sign of vagal stimulation, which can occur in response to gastric distension, vomiting, or suctioning. Vagal stimulation can slow down the heart rate and lower the blood pressure.
B. Hyperactive bowel sounds
Choice B: Hyperactive bowel sounds. This is not a manifestation of gastrointestinal perforation, but rather a sign of increased intestinal motility, which can occur in response to inflammation, infection, or irritation of the gastrointestinal tract. Hyperactive bowel sounds are loud, high-pitched, and frequent.
C. Report of epigastric fullness
Choice C: Report of epigastric fullness. This is not a manifestation of gastrointestinal perforation, but rather a sign of delayed gastric emptying, which can occur in response to gastric outlet obstruction, gastroparesis, or pyloric stenosis. Epigastric fullness is a feeling of pressure or discomfort in the upper abdomen after eating.
D. Severe upper abdominal pain
Choice D: Severe upper abdominal pain. This is a manifestation of gastrointestinal perforation, which is a life- threatening complication of peptic ulcer disease. Peptic ulcer disease is a condition that causes erosion and ulceration of the mucosal lining of the stomach or duodenum. If the ulcer penetrates through the wall of the gastrointestinal tract, it can cause perforation, which is a hole that allows gastric contents to leak into the peritoneal cavity. This can cause peritonitis, which is an inflammation and infection of the peritoneum. Peritonitis can cause severe upper abdominal pain, which may radiate to the shoulder or back. The pain may be sudden, sharp, and constant.
Full Explanation
Choice A: Bradycardia. This is not a manifestation of gastrointestinal perforation, but rather a sign of vagal stimulation, which can occur in response to gastric distension, vomiting, or suctioning. Vagal stimulation can slow down the heart rate and lower the blood pressure.
Choice B: Hyperactive bowel sounds. This is not a manifestation of gastrointestinal perforation, but rather a sign of increased intestinal motility, which can occur in response to inflammation, infection, or irritation of the gastrointestinal tract. Hyperactive bowel sounds are loud, high-pitched, and frequent.
Choice C: Report of epigastric fullness. This is not a manifestation of gastrointestinal perforation, but rather a sign of delayed gastric emptying, which can occur in response to gastric outlet obstruction, gastroparesis, or pyloric stenosis. Epigastric fullness is a feeling of pressure or discomfort in the upper abdomen after eating.
Choice D: Severe upper abdominal pain. This is a manifestation of gastrointestinal perforation, which is a life-threatening complication of peptic ulcer disease. Peptic ulcer disease is a condition that causes erosion and ulceration of the mucosal lining of the stomach or duodenum. If the ulcer penetrates through the wall of the gastrointestinal tract, it can cause perforation, which is a hole that allows gastric contents to leak into the peritoneal cavity. This can cause peritonitis, which is an inflammation and infection of the peritoneum. Peritonitis can cause severe upper abdominal pain, which may radiate to the shoulder or back. The pain may be sudden, sharp, and constant.