Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has fallen while getting out of bed and states, “I’m okay! I guess I should have called for help to the bathroom.” After assessing the client, the nurse notifies the provider.
Which of the following documentation should the nurse include in the client’s medical record?
A. An incident report was completed
The completion of an incident report should not be documented in the medical record. Incident reports are internal documents used for quality improvement and risk management, and mentioning them in the medical record could make them discoverable in legal proceedings.
B. There were no injuries sustained
While documenting the client’s physical condition is appropriate, stating "no injuries sustained" might be premature or subjective. Instead, the nurse should record specific observations, such as "client denies pain" or "no visible signs of injury noted."
C. The provider was notified
The nurse should document objective facts, such as notifying the provider, in the client’s medical record. This ensures accurate communication about the client's condition and the steps taken after the fall.
D. An incident report was forwarded to risk management
Referencing the incident report in the medical record is inappropriate. Incident reports are separate from the client’s medical record and should not be mentioned in the documentation.
This question is an excerpt from Nurse Dive's nursing test bank - Ivytech Fundamental Proctored Exam 2. Take the full exam now
Full Explanation
Correct Answer: C
C. The provider was notified. The nurse should document objective facts, such as notifying the provider, in the client’s medical record. This ensures accurate communication about the client's condition and the steps taken after the fall.
Incorrect answers:
A. "An incident report was completed." The completion of an incident report should not be documented in the medical record. Incident reports are internal documents used for quality improvement and risk management, and mentioning them in the medical record could make them discoverable in legal proceedings.
B. "There were no injuries sustained." While documenting the client’s physical condition is appropriate, stating "no injuries sustained" might be premature or subjective. Instead, the nurse should record specific observations, such as "client denies pain" or "no visible signs of injury noted."
D. "An incident report was forwarded to risk management. Referencing the incident report in the medical record is inappropriate. Incident reports are separate from the client’s medical record and should not be mentioned in the documentation.
Similar Questions
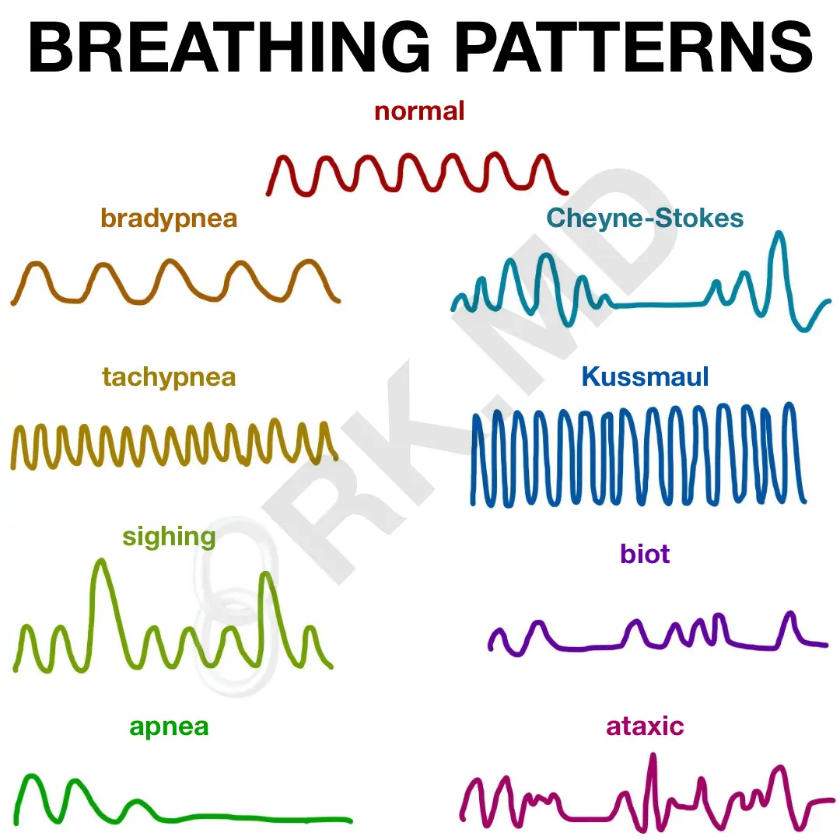
The nurse notes documentation that a client is exhibiting Cheyne-Stokes respirations. On assessment, what finding would the nurse expect?
A. Regular deep respirations interspersed with periods of apnea
Regular deep respirations interspersed with periods of apnea:This describes periodic breathing, which is different from Cheyne-Stokes respirations. Periodic breathing consists of regular cycles of deep respirations followed by periods of apnea.
B. A pattern of crescendo-decrescendo respirations followed by a period of apnea
A pattern of crescendo-decrescendo respirations followed by a period of apneaCheyne-Stokes respirations are characterized by a pattern of crescendo-decrescendo respirations, meaning that the depth and rate of breathing gradually increase and then decrease. This is followed by a period of apnea, during which there is a temporary cessation of breathing. The cycle then repeats.
C. Patient breathing less than 10 breaths per minute
Patient breathing less than 10 breaths per minute: This describes bradypnea, which is an abnormally slow respiratory rate. Cheyne-Stokes respirations involve rhythmic, cyclical changes in respiratory rate and depth.
D. Patient breathing shallow and more than 24 breaths per minute
Patient breathing shallow and more than 24 breaths per minute:This describes tachypnea, which is an abnormally fast respiratory rate. Cheyne-Stokes respirations are characterized by a distinct pattern of alternating crescendo-decrescendo respirations followed by apnea.
Full Explanation
A. Regular deep respirations interspersed with periods of apnea:
This describes periodic breathing, which is different from Cheyne-Stokes respirations. Periodic breathing consists of regular cycles of deep respirations followed by periods of apnea.
B. A pattern of crescendo-decrescendo respirations followed by a period of apnea
Cheyne-Stokes respirations are characterized by a pattern of crescendo-decrescendo respirations, meaning that the depth and rate of breathing gradually increase and then decrease. This is followed by a period of apnea, during which there is a temporary cessation of breathing. The cycle then repeats.
C. Patient breathing less than 10 breaths per minute:
This describes bradypnea, which is an abnormally slow respiratory rate. Cheyne-Stokes respirations involve rhythmic, cyclical changes in respiratory rate and depth.
D. Patient breathing shallow and more than 24 breaths per minute:
This describes tachypnea, which is an abnormally fast respiratory rate. Cheyne-Stokes respirations are characterized by a distinct pattern of alternating crescendo-decrescendo respirations followed by apnea.
A nurse is assessing for cyanosis in a client who has dark skin. Which of the following sites should the nurse examine to identify cyanosis in this client?
A. Dorsal surface of the foot
Dorsal surface of the foot:The skin on the dorsal surface of the foot may have more pigmentation, making it potentially more challenging to detect cyanosis in individuals with dark skin.
B. Pinnae of the ears
Pinnae of the ears:The ears may have variable pigmentation, and the presence of hair can affect the visibility of cyanosis. The skin on the pinnae may not be as thin as the skin on the dorsal surface of the hand.
C. Dorsal surface of the hand
Dorsal surface of the hand When assessing for cyanosis in a client with dark skin, the nurse should examine areas with less pigmentation or areas where the skin is thin. The dorsal surface of the hand is often a suitable site, as it is less pigmented and can show bluish discoloration if cyanosis is present.
D. Conjunctivae
Conjunctivae:The conjunctivae (the mucous membranes lining the inner surface of the eyelids and covering the white part of the eyes) are not a reliable site for assessing cyanosis in individuals with dark skin. Mucous membranes may not show cyanosis as prominently as the skin.
Full Explanation
A. Dorsal surface of the foot:
The skin on the dorsal surface of the foot may have more pigmentation, making it potentially more challenging to detect cyanosis in individuals with dark skin.
B. Pinnae of the ears:
The ears may have variable pigmentation, and the presence of hair can affect the visibility of cyanosis. The skin on the pinnae may not be as thin as the skin on the dorsal surface of the hand.
C. Dorsal surface of the hand
When assessing for cyanosis in a client with dark skin, the nurse should examine areas with less pigmentation or areas where the skin is thin. The dorsal surface of the hand is often a suitable site, as it is less pigmented and can show bluish discoloration if cyanosis is present.
D. Conjunctivae:
The conjunctivae (the mucous membranes lining the inner surface of the eyelids and covering the white part of the eyes) are not a reliable site for assessing cyanosis in individuals with dark skin. Mucous membranes may not show cyanosis as prominently as the skin.
A nurse is completing the initial admission assessment and history for a critical client. Which of the following is the priority action for the nurse to take?
A. Develop a plan of care for the client
Develop a plan of care for the client:Developing a plan of care is essential, but it should be informed by the client's current condition, diagnosis, and code status. Documenting the code status is a foundational step.
B. Provide a schedule of visiting hours to the client’s family
Provide a schedule of visiting hours to the client’s family:While facilitating family involvement is important, it is not the top priority during the initial admission assessment. Ensuring the client's safety and understanding their code status takes precedence.
C. Teach the client about his diagnosis
Teach the client about his diagnosis: Patient education is important, but in a critical situation, the priority is to assess and document key information, including the code status. Education can follow once the immediate priorities are addressed.
D. Document the client’s code status
Document the client’s code statusWhen conducting the initial admission assessment for a critical client, the priority action is to document the client's code status. Code status refers to the set of directives given by the client or their legal representative regarding the use of cardiopulmonary resuscitation (CPR) and other life-sustaining measures in the event of a cardiac or respiratory arrest.Understanding and documenting the client's code status is crucial for informing the healthcare team about the client's preferences for resuscitation efforts. This information guides the team in providing care that aligns with the client's wishes and values.
Full Explanation
A. Develop a plan of care for the client:
Developing a plan of care is essential, but it should be informed by the client's current condition, diagnosis, and code status. Documenting the code status is a foundational step.
B. Provide a schedule of visiting hours to the client’s family:
While facilitating family involvement is important, it is not the top priority during the initial admission assessment. Ensuring the client's safety and understanding their code status takes precedence.
C. Teach the client about his diagnosis:
Patient education is important, but in a critical situation, the priority is to assess and document key information, including the code status. Education can follow once the immediate priorities are addressed.
D. Document the client’s code status
When conducting the initial admission assessment for a critical client, the priority action is to document the client's code status. Code status refers to the set of directives given by the client or their legal representative regarding the use of cardiopulmonary resuscitation (CPR) and other life-sustaining measures in the event of a cardiac or respiratory arrest.
Understanding and documenting the client's code status is crucial for informing the healthcare team about the client's preferences for resuscitation efforts. This information guides the team in providing care that aligns with the client's wishes and values.