Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has paranoid schizophrenia and believes that they are being followed by FBI agents who are pretending to be psychiatric staff.
Which of the following responses should the nurse make?
A. The psychiatric staff is not FBI. They are here to help you.
The nurse should not deny the client's beliefs or try to convince them that they are wrong. This can cause the client to feel invalidated and may make them less likely to trust the nurse.
B. This must be very frightening for you. Let's talk more about it.
It is important for the nurse to acknowledge the client's fears and show empathy towards them. By saying "This must be very frightening for you," the nurse validates the client's feelings and shows that they are being heard. Additionally, by suggesting that they talk more about it, the nurse can work towards building a therapeutic relationship with the client and gain more insight into their thought processes.
C. What makes you think the staff is following you?
While it is important to understand the client's perspective, this question may come off as confrontational and accusatory.
D. Why do you feel the staff is the FBI?
Similarly, this question may be perceived as confrontational and may make the client defensive. It is important to approach the client with empathy and understanding rather than skepticism.
This question is an excerpt from Nurse Dive's nursing test bank - PN Comprehensive Predictor PN 2020 Proctored Exam. Take the full exam now
Full Explanation
b. This must be very frightening for you. Let's talk more about it.
It is important for the nurse to acknowledge the client's fears and show empathy towards them. By saying "This must be very frightening for you," the nurse validates the client's feelings and shows that they are being heard.
Additionally, by suggesting that they talk more about it, the nurse can work towards building a therapeutic relationship with the client and gain more insight into their thought processes.
The other options are not appropriate because:
a. The nurse should not deny the client's beliefs or try to convince them that they are wrong. This can cause
the client to feel invalidated and may make them less likely to trust the nurse.
c. While it is important to understand the client's perspective, this question may come off as confrontational and accusatory.
d. Similarly, this question may be perceived as confrontational and may make the client defensive. It is important to approach the client with empathy and understanding rather than skepticism.

Similar Questions
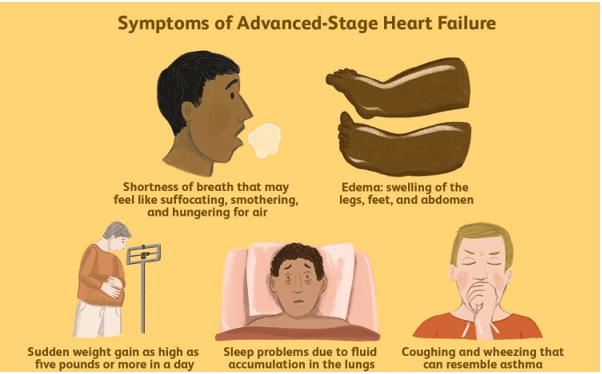
A nurse is reinforcing teaching about advance directives with a client who has end-stage heart failure.
Which of the following statements by the client indicates an understanding of the teaching?
A. I should discuss this document with my family after I sign it.
Advance directives are legal documents that allow an individual to specify the type of medical care they want to receive in case they become unable to make their own decisions. It is important for the client to discuss their wishes with their family members or loved ones so that they are aware of the client's desires and can act accordingly in case of an emergency.
B. I am not allowed to change my mind once I sign this document.
The client can change their mind about their advance directive at any time and for any reason. It is important for the client to review their advance directive periodically and make changes as necessary.
C. An atorney will need to notarize this document for it to be valid.
While some states require advance directives to be notarized or witnessed, not all states do. It is important for the client to check with their state's laws regarding advance directives to ensure that their document is legally binding.
D. My partner needs to be present when I sign this document.
While it is recommended for the client to have a witness present when signing their advance directive, it does not have to be their partner. The witness should be someone who is not a family member, healthcare provider, or beneficiary of the client's estate.
Full Explanation
a. "I should discuss this document with my family after I sign it"
Advance directives are legal documents that allow an individual to specify the type of medical care they want to receive in case they become unable to make their own decisions. It is important for the client to discuss their wishes with their family members or loved ones so that they are aware of the client's desires and can act accordingly in case of an emergency.
b. "I am not allowed to change my mind once I sign this document" is incorrect. The client can change their mind about their advance directive at any time and for any reason. It is important for the client to review their advance directive periodically and make changes as necessary.
c. "An atorney will need to notarize this document for it to be valid" is also incorrect. While some states require advance directives to be notarized or witnessed, not all states do. It is important for the client to check with their state's laws regarding advance directives to ensure that their document is legally binding.
d. "My partner needs to be present when I sign this document" is not necessarily true. While it is recommended for the client to have a witness present when signing their advance directive, it does not have to be their partner. The witness should be someone who is not a family member, healthcare provider, or beneficiary of the client's estate.
A nurse is reinforcing teaching with a client who has diabetes mellitus about a 24-hour creatinine clearance test.
Which of the following statements should the nurse include in the teaching?
A. You should eat a protein-rich diet during the collection period.
A protein-rich diet can affect the creatinine levels in the urine, which can result in inaccurate test results. Therefore, the nurse should advise the client to avoid a protein-rich diet during the collection period.
B. You should record your blood glucose level each time you void.
Blood glucose levels are not relevant to a 24-hour creatinine clearance test. Therefore, the nurse should not ask the client to record their blood glucose level each time they void.
C. You can begin collection of urine after discarding your first morning void.
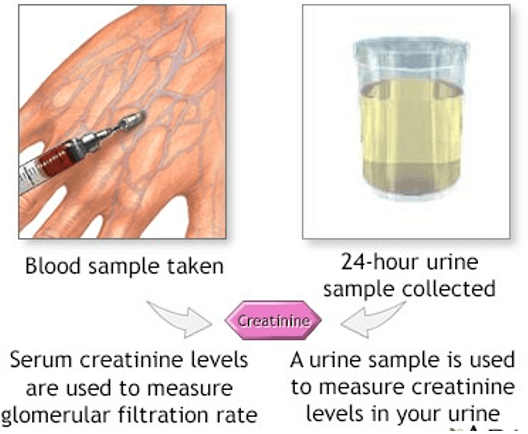
A 24-hour creatinine clearance test is used to evaluate how well the kidneys are functioning by measuring the amount of creatinine in the blood and urine over a 24-hour period. During the test, the client is asked to discard their first morning void and then collect all urine for the next 24 hours.
D. You can cleanse your perineal area with an antiseptic towel each time before you void.
An antiseptic towel to cleanse the perineal area can also affect the test results by introducing contaminants into the urine sample. Therefore, the nurse should advise the client to cleanse the perineal area with soap and water or an alcohol wipe.
Full Explanation
C, "You can begin collection of urine after discarding your first morning void."
A 24-hour creatinine clearance test is used to evaluate how well the kidneys are functioning by measuring the amount of creatinine in the blood and urine over a 24-hour period. During the test, the client is asked to discard their first morning void and then collect all urine for the next 24 hours.
Option A is incorrect because a protein-rich diet can affect the creatinine levels in the urine, which can result in inaccurate test results. Therefore, the nurse should advise the client to avoid a protein-rich diet during the collection period.
Option B is incorrect because blood glucose levels are not relevant to a 24-hour creatinine clearance test. Therefore, the nurse should not ask the client to record their blood glucose level each time they void.
Option D is incorrect because using an antiseptic towel to cleanse the perineal area can also affect the test results by introducing contaminants into the urine sample. Therefore, the nurse should advise the client to cleanse the perineal area with soap and water or an alcohol wipe.
A nurse in an adult day care facility is contributing to the plan of care for a client whose family reports recent confusion and memory loss.
Which of the following strategies should the nurse include in the plan?
A. Maintain low-level lights in common areas.
Low-level lighting can increase confusion and the risk of falls, especially for clients with memory loss. It is important to have adequate lighting to promote a safe environment and help with orientation. Well-lit areas can reduce disorientation and anxiety in clients who are confused or have memory issues.
B. Give the client several meal options at lunchtime.
For clients with memory loss and confusion, it is better to provide simple choices or pre-selected meals to reduce decision-making stress and confusion.
C. Confront the client regarding inappropriate behavior.
Confronting a client with memory loss or confusion about inappropriate behavior can increase agitation, anxiety, and defensive reactions.
D. Use symbols in the communal room signage.
Symbols and pictures can help clients with memory loss navigate their environment more easily because they may have difficulty reading or comprehending written language. Visual cues such as symbols in signage can improve orientation and independence, helping the client feel more comfortable in their surroundings.
Full Explanation
A. Maintain low-level lights in common areas. Low-level lighting can increase confusion and the risk of falls, especially for clients with memory loss. It is important to have adequate lighting to promote a safe environment and help with orientation. Well-lit areas can reduce disorientation and anxiety in clients who are confused or have memory issues.
B. Give the client several meal options at lunchtime. For clients with memory loss and confusion, it is better to provide simple choices or pre-selected meals to reduce decision-making stress and confusion.
C. Confront the client regarding inappropriate behavior. Confronting a client with memory loss or confusion about inappropriate behavior can increase agitation, anxiety, and defensive reactions.
D. Use symbols in the communal room signage. Symbols and pictures can help clients with memory loss navigate their environment more easily because they may have difficulty reading or comprehending written language. Visual cues such as symbols in signage can improve orientation and independence, helping the client feel more comfortable in their surroundings.