Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
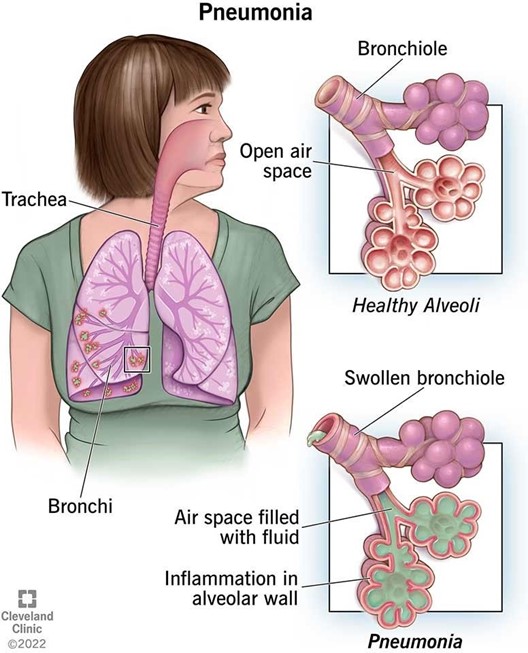
A nurse is caring for a client who has pneumonia. Which of the following actions should the nurse take to promote thinning of respiratory secretions?
A. Encourage coughing and deep breathing
Encourage coughing and deep breathing. This is beneficial for clearing the airways and preventing atelectasis, but it does not directly affect the viscosity of the secretions.
B. Encourage regular use of the incentive spirometer
Encourage regular use of the incentive spirometer. This is helpful for expanding the lungs and preventing complications such as pneumonia or pleural effusion, but it does not influence the consistency of the secretions.
C. Encourage the client to increase fluid intake
Increasing fluid intake helps to hydrate the mucous membranes and thin the respiratory secretions, which facilitates expectoration and improves gas exchange.
D. Encourage the client to ambulate frequently
Encourage the client to ambulate frequently. This is important for promoting circulation and mobility, but it does not have a significant effect on the thinning of the secretions.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 1. Take the full exam now
Full Explanation
Increasing fluid intake helps to hydrate the mucous membranes and thin the respiratory secretions, which facilitates expectoration and improves gas exchange.
- Encourage coughing and deep breathing. This is beneficial for clearing the airways and preventing atelectasis, but it does not directly affect the viscosity of the secretions.
- Encourage regular use of the incentive spirometer. This is helpful for expanding the lungs and preventing complications such as pneumonia or pleural effusion, but it does not influence the consistency of the secretions.
- Encourage the client to ambulate frequently. This is important for promoting circulation and mobility, but it does not have a significant effect on the thinning of the secretions.
Similar Questions
A nurse is preparing to titrate morphine 6 mg via IV bolus to a client. The amount available is morphine 8 mg/mL. How many mL should the nurse administer per dose?
(Round the answer to the nearest hundredth. Use a leading zero if it applies. Do not use a trailing zero.)
Full Explanation
To calculate the volume of solution, use the formula:
mL = (desired dose in mg / available dose in mg) x 1 mL
Plug in the given values:
mL = (6 mg / 8 mg) x 1 mL
Simplify and solve:
mL = 0.75 x 1 mL
mL = 0.75 mL
Round to the nearest hundredth and add a leading zero if needed:
mL = 0.75 mL
A nurse is caring for a client who is unconscious and has a breathing pattern characterized by alternating periods of hyperventilation and apnea. The nurse should document that the client has which of the following respiratory alterations?
A. Stridor
A) Stridor: Stridor is a high-pitched, wheezing sound resulting from disrupted airflow in the upper airway. It is not characterized by alternating periods of hyperventilation and apnea, making this choice incorrect.
B. Kussmaul respirations
B) Kussmaul respirations: Kussmaul respirations are deep, labored breaths typically associated with metabolic acidosis, such as diabetic ketoacidosis. These respirations do not exhibit alternating periods of hyperventilation and apnea, so this option is not applicable.
C. Apneustic respirations
C) Apneustic respirations: Apneustic respirations are characterized by prolonged inhalation followed by a prolonged pause before exhalation. This pattern does not align with the alternating hyperventilation and apnea described, making it an incorrect choice.
D. Cheyne-Stokes respirations
D) Cheyne-Stokes respirations: Cheyne-Stokes respirations are characterized by a cyclical pattern of increasing depth and rate of breathing followed by a gradual decrease in depth and a period of apnea. This description matches the client's breathing pattern of alternating hyperventilation and apnea, making this the correct answer.
Full Explanation
Answer: D. Cheyne-Stokes respirations
Rationale:
A) Stridor: Stridor is a high-pitched, wheezing sound resulting from disrupted airflow in the upper airway. It is not characterized by alternating periods of hyperventilation and apnea, making this choice incorrect.
B) Kussmaul respirations: Kussmaul respirations are deep, labored breaths typically associated with metabolic acidosis, such as diabetic ketoacidosis. These respirations do not exhibit alternating periods of hyperventilation and apnea, so this option is not applicable.
C) Apneustic respirations: Apneustic respirations are characterized by prolonged inhalation followed by a prolonged pause before exhalation. This pattern does not align with the alternating hyperventilation and apnea described, making it an incorrect choice.
D) Cheyne-Stokes respirations: Cheyne-Stokes respirations are characterized by a cyclical pattern of increasing depth and rate of breathing followed by a gradual decrease in depth and a period of apnea. This description matches the client's breathing pattern of alternating hyperventilation and apnea, making this the correct answer.
A nurse in an urgent care center is caring for a client who is having an acute asthma exacerbation. Which of the following actions is the nurse's highest priority?
A. Administering a nebulized beta-adrenergic
A) Administering a nebulized beta-adrenergic: In the case of an acute asthma exacerbation, administering a nebulized beta-adrenergic agonist (such as albuterol) is the highest priority. These medications act quickly to relax bronchial smooth muscle, dilate airways, and improve airflow. This intervention directly addresses the underlying bronchospasm and helps to alleviate the acute symptoms of asthma.
B. Providing immediate rest for the client
B) Providing immediate rest for the client: While rest is important in managing an acute asthma exacerbation, it is not the immediate priority. Addressing the airway obstruction with appropriate medications is crucial for stabilizing the client's condition before focusing on comfort measures such as rest.
C. Positioning the client in high-Fowler's
C) Positioning the client in high-Fowler's: Positioning the client in a high-Fowler's position can help improve lung expansion and facilitate breathing. However, this action is secondary to administering medication that can relieve the acute symptoms of bronchoconstriction. The medication should be administered first to rapidly address the exacerbation.
D. Initiating oxygen therapy
D) Initiating oxygen therapy: Oxygen therapy might be necessary if the client shows signs of hypoxemia or severe respiratory distress. However, the immediate priority is to address the bronchospasm with a nebulized beta-adrenergic agonist to improve airflow. Once the acute bronchospasm is managed, oxygen therapy can be implemented if needed to support oxygen saturation.
Full Explanation
Answer: A
Rationale:
A) Administering a nebulized beta-adrenergic:
In the case of an acute asthma exacerbation, administering a nebulized beta-adrenergic agonist (such as albuterol) is the highest priority. These medications act quickly to relax bronchial smooth muscle, dilate airways, and improve airflow. This intervention directly addresses the underlying bronchospasm and helps to alleviate the acute symptoms of asthma.
B) Providing immediate rest for the client:
While rest is important in managing an acute asthma exacerbation, it is not the immediate priority. Addressing the airway obstruction with appropriate medications is crucial for stabilizing the client's condition before focusing on comfort measures such as rest.
C) Positioning the client in high-Fowler's:
Positioning the client in a high-Fowler's position can help improve lung expansion and facilitate breathing. However, this action is secondary to administering medication that can relieve the acute symptoms of bronchoconstriction. The medication should be administered first to rapidly address the exacerbation.
D) Initiating oxygen therapy:
Oxygen therapy might be necessary if the client shows signs of hypoxemia or severe respiratory distress. However, the immediate priority is to address the bronchospasm with a nebulized beta-adrenergic agonist to improve airflow. Once the acute bronchospasm is managed, oxygen therapy can be implemented if needed to support oxygen saturation.