Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who has valvular heart disease and is at risk for developing left-sided heart failure. Which of the following manifestations should alert the nurse that the client is developing this condition?
A. Weight gain
Weight gain is not a manifestation of left-sided heart failure. Weight gain is more likely to occur in right- sided heart failure, as the blood backs up in the systemic circulation and causes fluid retention and edema in the body.
B. Anorexia
Anorexia is not a manifestation of left-sided heart failure. Anorexia is a loss of appetite, which can have many causes, such as psychological disorders, infections, medications, or cancer. Left-sided heart failure does not directly affect appetite, but it can cause nausea, fatigue, and weakness.
C. Distended abdomen
Distended abdomen is not a manifestation of left-sided heart failure. Distended abdomen is more likely to occur in right-sided heart failure, as the blood backs up in the portal vein and causes increased pressure in the liver and spleen. This can lead to hepatomegaly, splenomegaly, ascites, and varices.
D. Breathlessness
Breathlessness is a manifestation of left-sided heart failure. Breathlessness, or dyspnea, is a sensation of difficulty breathing or shortness of breath. Breathlessness occurs in left-sided heart failure, as the blood backs up in the lungs and causes pulmonary congestion and edema. This impairs gas exchange and reduces oxygen delivery to the tissues.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg 2 Proctored Exam. Take the full exam now
Full Explanation
Choice A: Weight gain is not a manifestation of left-sided heart failure. Weight gain is more likely to occur in right-sided heart failure, as the blood backs up in the systemic circulation and causes fluid retention and edema in the body.
Choice B: Anorexia is not a manifestation of left-sided heart failure. Anorexia is a loss of appetite, which can have many causes, such as psychological disorders, infections, medications, or cancer. Left-sided heart failure does not directly affect appetite, but it can cause nausea, fatigue, and weakness.
Choice C: A distended abdomen is not a manifestation of left-sided heart failure. A distended abdomen is more likely to occur in right-sided heart failure, as the blood backs up in the portal vein and causes increased pressure in the liver and spleen. This can lead to hepatomegaly, splenomegaly, ascites, and varices.
Choice D: Breathlessness is a manifestation of left-sided heart failure. Breathlessness, or dyspnea, is a sensation of difficulty breathing or shortness of breath. Breathlessness occurs in left-sided heart failure, as the blood backs up in the lungs and causes pulmonary congestion and edema. This impairs gas exchange and reduces oxygen delivery to the tissues.
Similar Questions
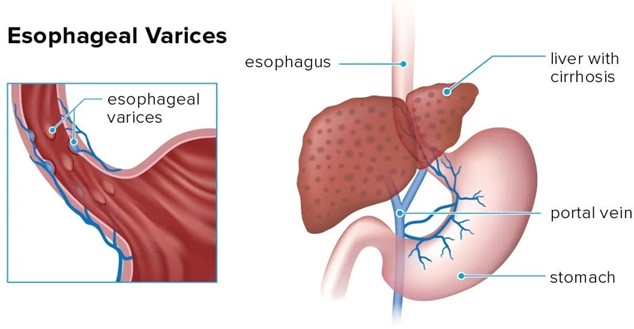
A nurse is caring for a client who was admited with bleeding esophageal varices and has an esophagogastric balloon tamponade with a Sengstaken-Blakemore tube to control the bleeding. Which of the following actions should the nurse take?
A. Provide frequent oral and nares care
Provide frequent oral and nares care is the correct action for the nurse to take. Oral and nares care can help prevent infection, dryness, and irritation of the mucous membranes, which can be damaged by the pressure and friction of the tube. The nurse should also monitor the tube position, secure it with tape, and keep scissors at the bedside in case of emergency deflation.
B. Keep the client in a supine position
Keep the client in a supine position is not the correct action for the nurse to take. The supine position can increase the risk of aspiration, regurgitation, and gastric distension, which can worsen the bleeding and compromise the airway. The nurse should elevate the head of the bed to at least 30 degrees and use a semi-Fowler's or high- Fowler's position.
C. Ambulate the client four times per day
Ambulate the client four times per day is not the correct action for the nurse to take. Ambulation can increase abdominal pressure and dislodge the tube, which can cause bleeding and perforation. The nurse should keep the client on bed rest and use passive range-of-motion exercises to prevent complications such as thromboembolism and muscle atrophy.
D. Encourage the client to consume clear liquids
Encourage the client to consume clear liquids is not the correct action for the nurse to take. Clear liquids can increase gastric volume and acidity, which can aggravate the bleeding and interfere with hemostasis. The nurse should maintain nothing-by-mouth status and provide intravenous fluids and nutrition as prescribed.
Full Explanation
Choice A: Provide frequent oral and nares care is the correct action for the nurse to take. Oral and nares care can help prevent infection, dryness, and irritation of the mucous membranes, which can be damaged by the pressure and friction of the tube. The nurse should also monitor the tube position, secure it with tape, and keep scissors at the bedside in case of emergency deflation.
Choice B: Keep the client in a supine position is not the correct action for the nurse to take. The supine position can increase the risk of aspiration, regurgitation, and gastric distension, which can worsen the bleeding and compromise the airway. The nurse should elevate the head of the bed to at least 30 degrees and use a semi-Fowler's or high-Fowler's position.
Choice C: Ambulating the client four times per day is not the correct action for the nurse to take. Ambulation can increase abdominal pressure and dislodge the tube, which can cause bleeding and perforation. The nurse should keep the client on bed rest and use passive range-of-motion exercises to prevent complications such as thromboembolism and muscle atrophy.
Choice D: Encouraging the client to consume clear liquids is not the correct action for the nurse to take. Clear liquids can increase gastric volume and acidity, which can aggravate the bleeding and interfere with hemostasis. The nurse should maintain a nothing-by-mouth status and provide intravenous fluids and nutrition as prescribed.
A nurse in the emergency department is monitoring a client who has a cervical spinal cord injury from a fall. The nurse should monitor the client for which of the following complications? (Select all that apply.)
A. Weakened gag reflex
Choice A: A cervical spinal cord injury can impair the function of cranial nerves, leading to a weakened gag reflex and an increased risk of aspiration.
B. Hyperthermia
Choice B: Patients with spinal cord injuries are more likely to experience poikilothermia (difficulty regulating body temperature), but this often results in hypothermia, not hyperthermia, due to the loss of autonomic temperature control.
C. Absence of bowel sounds
Choice C: Spinal shock, which often follows a spinal cord injury, can cause decreased or absent bowel sounds due to a temporary loss of autonomic function and decreased peristalsis.
D. Paralysis
Choice D: Depending on the level and severity of the injury, paralysis can occur, affecting motor function below the injury site. A cervical spinal cord injury may lead to quadriplegia (tetraplegia).
E. Polyuria
Choice E: Clients with spinal cord injuries are more likely to experience urinary retention, rather than polyuria, due to loss of bladder control and autonomic dysfunction. A foley catheter may be needed initially, followed by intermittent catheterization.
F. Hypotension
Choice F: Neurogenic shock, a potential complication of cervical spinal cord injuries, can cause hypotension due to the loss of sympathetic nervous system control over blood vessel tone, leading to vasodilation and bradycardia.
Full Explanation
Choice A: A cervical spinal cord injury can impair the function of cranial nerves, leading to a weakened gag reflex and an increased risk of aspiration.
Choice B: Patients with spinal cord injuries are more likely to experience poikilothermia (difficulty regulating body temperature), but this often results in hypothermia, not hyperthermia, due to the loss of autonomic temperature control.
Choice C: Spinal shock, which often follows a spinal cord injury, can cause decreased or absent bowel sounds due to a temporary loss of autonomic function and decreased peristalsis.
Choice D: Depending on the level and severity of the injury, paralysis can occur, affecting motor function below the injury site. A cervical spinal cord injury may lead to quadriplegia (tetraplegia).
Choice E: Clients with spinal cord injuries are more likely to experience urinary retention, rather than polyuria, due to loss of bladder control and autonomic dysfunction. A foley catheter may be needed initially, followed by intermittent catheterization.
Choice F: Neurogenic shock, a potential complication of cervical spinal cord injuries, can cause hypotension due to the loss of sympathetic nervous system control over blood vessel tone, leading to vasodilation and bradycardia.
A nurse is caring for a client who has increased intracranial pressure. Which of the following interventions should the nurse take?
A. Provide a brightly lit environment
Provide a brightly lit environment is not an intervention that the nurse should take. A brightly lit environment can stimulate the brain and increase intracranial pressure. The nurse should provide a quiet and dimly lit environment to reduce sensory stimuli and promote rest.
B. Elevate the head of the bed
Elevate the head of the bed is an intervention that the nurse should take. Elevating the head of the bed to 30 degrees can help reduce intracranial pressure by facilitating venous drainage from the brain and decreasing cerebral blood volume. The nurse should avoid flexing or extending the neck, which can impede blood flow and increase intracranial pressure.
C. Encourage a minimum intake of 2000 mL (67.6 oz) of clear fluids per day
Encourage a minimum intake of 2000 mL (67.6 oz) of clear fluids per day is not an intervention that the nurse should take. A high fluid intake can increase intracranial pressure by increasing blood volume and cerebral edema. The nurse should monitor fluid balance and restrict fluid intake as prescribed to maintain normal osmolality and prevent fluid overload.
D. Teach controlled coughing and deep breathing
Teach controlled coughing and deep breathing is not an intervention that the nurse should take. Coughing and deep breathing can increase intrathoracic pressure, which can increase intracranial pressure by reducing venous return from the brain. The nurse should avoid activities that can increase intrathoracic pressure, such as straining, sneezing, or blowing the nose. The nurse should also administer oxygen as prescribed to maintain adequate oxygenation and perfusion of the brain.
Full Explanation
Choice A: Provide a brightly lit environment is not an intervention that the nurse should take. A brightly lit environment can stimulate the brain and increase intracranial pressure. The nurse should provide a quiet and dimly lit environment to reduce sensory stimuli and promote rest.
Choice B: Elevate the head of the bed is an intervention that the nurse should take. Elevating the head of the bed to 30 degrees can help reduce intracranial pressure by facilitating venous drainage from the brain and decreasing cerebral blood volume. The nurse should avoid flexing or extending the neck, which can impede blood flow and increase intracranial pressure.
Choice C: Encourage a minimum intake of 2000 mL (67.6 oz) of clear fluids per day is not an intervention that the nurse should take. A high fluid intake can increase intracranial pressure by increasing blood volume and cerebral edema. The nurse should monitor fluid balance and restrict fluid intake as prescribed to maintain normal osmolality and prevent fluid overload.
Choice D: Teach controlled coughing and deep breathing is not an intervention that the nurse should take. Coughing and deep breathing can increase intrathoracic pressure, which can increase intracranial pressure by reducing venous return from the brain. The nurse should avoid activities that can increase intrathoracic pressure, such as straining, sneezing, or blowing the nose. The nurse should also administer oxygen as prescribed to maintain adequate oxygenation and perfusion of the brain.