Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a client who is 1 day postoperative following a total hip arthroplasty and is receiving heparin subcutaneously.
Which of the following adverse effects of the medication should the nurse report to the provider?
A. Weight gain
Is not a common adverse effect of heparin. Weight gain can be caused by various factors, but it is not directly related to heparin administration.
B. Bradycardia
Is not a common adverse effect of heparin. Bradycardia can be caused by other factors unrelated to heparin therapy and should be evaluated separately.
C. Epistaxis
Heparin is an anticoagulant medication used to prevent blood clot formation. One of the potential adverse effects of heparin therapy is bleeding. Epistaxis, or nosebleeds, can be a sign of abnormal bleeding and should be reported to the provider for further evaluation and adjustment of the treatment plan if necessary.
D. Anorexia
Is not typically associated with heparin therapy. Anorexia can have various causes, but it is not directly linked to heparin administration.
This question is an excerpt from Nurse Dive's nursing test bank - ATI PN Comprehensive Predictor 2023 - Proctored Exam 1. Take the full exam now
Full Explanation
Explanation
C. Epistaxis
Heparin is an anticoagulant medication used to prevent blood clot formation. One of the potential adverse effects of heparin therapy is bleeding. Epistaxis, or nosebleeds, can be a sign of abnormal bleeding and should be reported to the provider for further evaluation and adjustment of the treatment plan if necessary.
Weight gain in (option A) is not a common adverse effect of heparin. Weight gain can be caused by various factors, but it is not directly related to heparin administration.
Bradycardia (slow heart rate) in (option B) is not a common adverse effect of heparin. Bradycardia can be caused by other factors unrelated to heparin therapy and should be evaluated separately.
Anorexia (loss of appetite) in (option D) is not typically associated with heparin therapy. Anorexia can have various causes, but it is not directly linked to heparin administration.
Therefore, the nurse should report the occurrence of epistaxis (option C) to the healthcare provider as a potential adverse effect of heparin therapy in the client.
Similar Questions
A nurse is reinforcing teaching with the parents of a toddler who has a new diagnosis of asthma and a prescription for montelukast.
Which of the following instructions should the nurse include in the teaching?
A. Administer the medication to the toddler each evening.
Montelukast is a long-term control medication used for the management of asthma in both children and adults. It is typically taken once daily in the evening to provide continuous asthma control. Consistency in taking the medication is important to maintain its effectiveness.
B. Provide an additional dose of the medication prior to physical activity.
Is not a standard recommendation for montelukast use. Montelukast is not a rescue medication and does not provide immediate relief for asthma symptoms triggered by physical activity. In such cases, a short-acting bronchodilator medication, such as albuterol, is commonly used prior to physical activity.
C. Mix the medication in juice prior to administration.
Is not recommended unless specifically instructed by the healthcare provider or indicated in the medication instructions. Montelukast is available in various formulations, including chewable tablets and granules, which can be taken directly or mixed with certain foods or liquids. However, the specific instructions should be followed as provided by the healthcare provider or medication label.
D. Administer the medication when the toddler has an acute asthma attack.
Has an acute asthma attack is not the intended use of montelukast. Montelukast is a long-term control medication aimed at preventing asthma symptoms and maintaining asthma control over time. For acute asthma attacks, a short-acting bronchodilator medication is typically used.
Full Explanation
Explanation
A. Administer the medication to the toddler each evening.
Montelukast is a long-term control medication used for the management of asthma in both children and adults. It is typically taken once daily in the evening to provide continuous asthma control. Consistency in taking the medication is important to maintain its effectiveness.
Providing an additional dose of the medication prior to physical activity in (option B) is not a standard recommendation for montelukast use. Montelukast is not a rescue medication and does not provide immediate relief for asthma symptoms triggered by physical activity. In such cases, a short-acting bronchodilator medication, such as albuterol, is commonly used prior to physical activity.
Mixing the medication in juice prior to administration in (option C) is not recommended unless specifically instructed by the healthcare provider or indicated in the medication instructions.
Montelukast is available in various formulations, including chewable tablets and granules, which can be taken directly or mixed with certain foods or liquids. However, the specific instructions should be followed as provided by the healthcare provider or medication label.
Administering the medication when the toddler in (option D) has an acute asthma attack is not the intended use of montelukast. Montelukast is a long-term control medication aimed at preventing asthma symptoms and maintaining asthma control over time. For acute asthma attacks, a short-acting bronchodilator medication is typically used.
Therefore, the nurse should instruct the parents to administer the medication to the toddler each evening (option A) as part of the routine, long-term management of asthma.
A nurse is reinforcing teaching about home safety precautions with the parents of a 3-month- old infant.
Which of the following instructions should the nurse include in the teaching?
A. Place no more than one small pillow in the crib.
The American Academy of Pediatrics (AAP) recommends that infants should sleep on a firm and flat surface without any pillows, blankets, or soft bedding. These items can pose a suffocation risk. So, the nurse should advise against using any pillows in the crib.
B. Remove bibs when the infant is going to sleep.
This is a good recommendation. Bibs can be a choking hazard during sleep. Removing them ensures the baby’s safety and reduces the risk of accidental suffocation
C. Make sure the crib mattress is soft.
Is not recommended. The crib mattress should be firm to provide a safe sleeping surface for the infant. Soft mattresses can increase the risk of suffocation.
D. Start using a highchair for feedings.
Is not typically necessary or developmentally appropriate. At this age, infants are typically fed while being held in a caregiver's arms or in a reclined position, such as in a baby bouncer or supported seat.
Full Explanation
Correct answer: B
A. Place no more than one small pillow in the crib
The American Academy of Pediatrics (AAP) recommends that infants should sleep on a firm and flat surface without any pillows, blankets, or soft bedding. These items can pose a suffocation risk. So, the nurse should advise against using any pillows in the crib.
B. This is a good recommendation. Bibs can be a choking hazard during sleep. Removing them ensures the baby’s safety and reduces the risk of accidental suffocation
C. Making sure the crib mattress is soft in (option C) is not recommended. The crib mattress should be firm to provide a safe sleeping surface for the infant. Soft mattresses can increase the risk of suffocation.
D. Starting to use a highchair for feedings at 3 months old in (option D) is not typically necessary or developmentally appropriate. At this age, infants are typically fed while being held in a caregiver's arms or in a reclined position, such as in a baby bouncer or supported seat.
A nurse is collecting data from a client who has heart failure. The nurse notes the client has crackles in the bases of the lungs, shortness of breath, and a respiratory rate of 24/min.
Which of the following actions should the nurse take?
A. Instruct the client to cough every 4 hr.
Is not the priority action in this situation. Coughing may not effectively address the underlying cause of pulmonary congestion and may not provide immediate relief for the client.
B. Encourage the client to ambulate to loosen secretions.
Is not the priority action in this situation. While ambulation can be beneficial for overall health, the client's symptoms of pulmonary congestion require immediate attention to improve respiratory status.
C. Increase the client's intake of oral fluids.
Is not the priority action in this situation. While maintaining adequate hydration is important, excessive fluid intake can worsen the symptoms of heart failure and contribute to further fluid accumulation in the lungs.
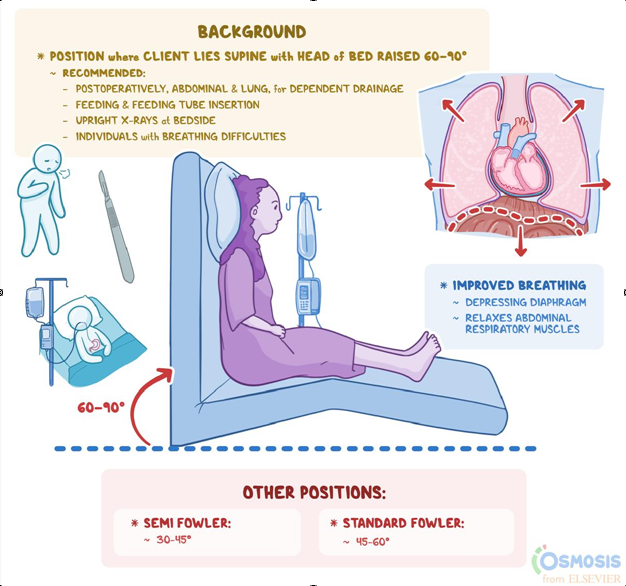
D. Maintain the client in high-Fowler's position.
Crackles in the bases of the lungs, shortness of breath, and an increased respiratory rate are signs of pulmonary congestion, which is commonly seen in heart failure. Maintaining the client in a high-Fowler's position, with the head of the bed elevated to a 45-60-degree angle, helps reduce venous return to the heart, decreases fluid accumulation in the lungs, and improves breathing comfort for the client.
Full Explanation
Explanation
D. Maintain the client in high-Flower’s position
Crackles in the bases of the lungs, shortness of breath, and an increased respiratory rate are signs of pulmonary congestion, which is commonly seen in heart failure. Maintaining the client in a high-Fowler's position, with the head of the bed elevated to a 45-60-degree angle, helps reduce venous return to the heart, decreases fluid accumulation in the lungs, and improves breathing comfort for the client.
The other options are not appropriate actions for the client's condition:
Instructing the client to cough every 4 hours in (option A) is not the priority action in this situation. Coughing may not effectively address the underlying cause of pulmonary congestion and may not provide immediate relief for the client.
Encouraging the client to ambulate to loosen secretions in (option B) is not the priority action in this situation. While ambulation can be beneficial for overall health, the client's symptoms of pulmonary congestion require immediate attention to improve respiratory status.
Increasing the client's intake of oral fluids in (option C) is not the priority action in this situation. While maintaining adequate hydration is important, excessive fluid intake can worsen the symptoms of heart failure and contribute to further fluid accumulation in the lungs.
Therefore, the nurse should maintain the client in high-Fowler's position (option D) to promote optimal lung function and improve breathing comfort. It is important to promptly notify the healthcare provider of the client's condition for further assessment and intervention.