Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
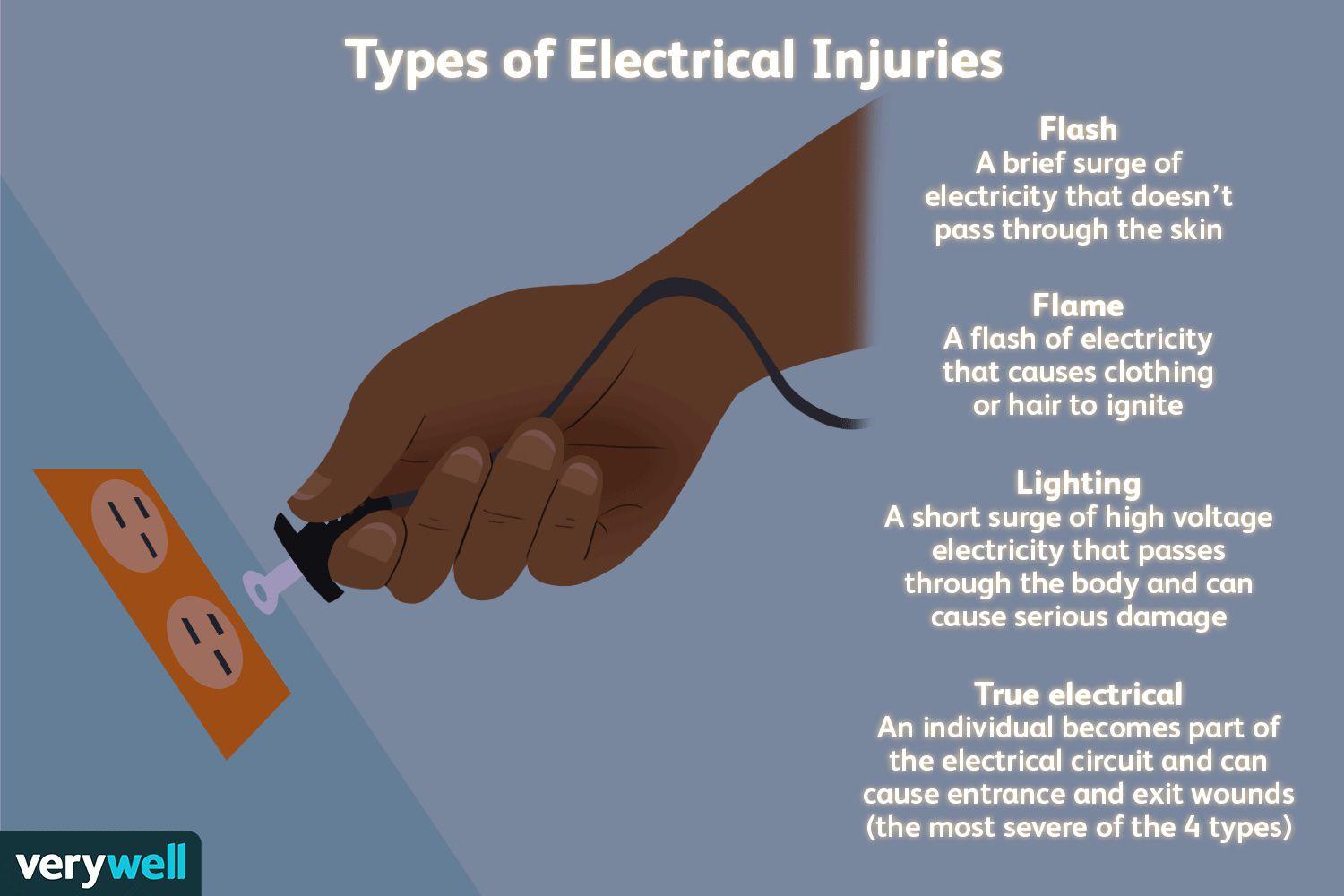
A nurse is caring for a client with an electrical burn. The client states that since the wound on the skin is small, the burn must not be too bad. Which of the following is the best response by the nurse?
A. Electrical burns can have small amounts of skin damage, but more extensive damage beneath the skin.
Electrical burns can have small amounts of skin damage, but more extensive damage beneath the skin.This response is the best choice because it educates the client about the potential for deeper tissue damage associated with electrical burns. It acknowledges that while the burn on the skin may appear small, the damage underneath could be more extensive, affecting muscles, nerves, and blood vessels.
B. Electrical burns commonly cause reddened/purplish skin without blistering.
Electrical burns commonly cause reddened/purplish skin without blistering.This statement is not the best response because it focuses solely on the appearance of the skin without addressing the potential for deeper tissue damage. While it is true that electrical burns can present with reddened or purplish skin without blistering, this response does not provide comprehensive information about the nature and severity of electrical burns.
C. Electrical burns typically are minor.
Electrical burns typically are minor. This response is incorrect because it downplays the seriousness of electrical burns. While some electrical burns may indeed be minor, others can cause significant tissue damage and complications. It's important for the nurse to educate the client about the range of severity that electrical burns can present.
D. Electrical burns usually cause much more skin damage than what can be seen on your skin.
Electrical burns usually cause much more skin damage than what can be seen on your skin.This statement is partially accurate but does not provide as much information as choice A. While it acknowledges that electrical burns can cause more damage than what is visible on the skin's surface, it doesn't emphasize the potential for deeper tissue damage as effectively as choice A does.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Lpn Med Surg Cohort 6 Proctored Exam. Take the full exam now
Full Explanation
A. Electrical burns can have small amounts of skin damage, but more extensive damage beneath the skin.
This response is the best choice because it educates the client about the potential for deeper tissue damage associated with electrical burns. It acknowledges that while the burn on the skin may appear small, the damage underneath could be more extensive, affecting muscles, nerves, and blood vessels.
B. Electrical burns commonly cause reddened/purplish skin without blistering.
This statement is not the best response because it focuses solely on the appearance of the skin without addressing the potential for deeper tissue damage. While it is true that electrical burns can present with reddened or purplish skin without blistering, this response does not provide comprehensive information about the nature and severity of electrical burns.
C. Electrical burns typically are minor.
This response is incorrect because it downplays the seriousness of electrical burns. While some electrical burns may indeed be minor, others can cause significant tissue damage and complications. It's important for the nurse to educate the client about the range of severity that electrical burns can present.
D. Electrical burns usually cause much more skin damage than what can be seen on your skin.
This statement is partially accurate but does not provide as much information as choice A. While it acknowledges that electrical burns can cause more damage than what is visible on the skin's surface, it doesn't emphasize the potential for deeper tissue damage as effectively as choice A does.
Similar Questions
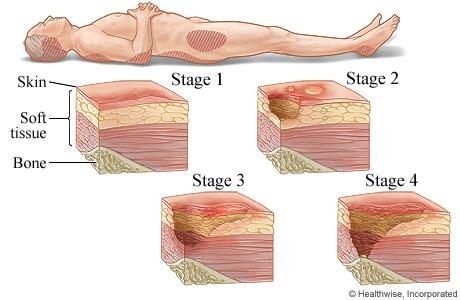
A nurse is caring for a client that is immobile. The nurse recognizes that the appearance of non-blanchable erythema on the heels most likely indicates which of the following stages of pressure injuries?
A. Stage III pressure injury
Stage III pressure injuryStage III pressure injuries involve full-thickness skin loss, extending into the subcutaneous tissue but not through the fascia. These wounds typically present as deep craters and may involve undermining or tunneling. Non-blanchable erythema alone without visible skin loss is not characteristic of a Stage III pressure injury.
B. Stage IV pressure injury
Stage IV pressure injuryStage IV pressure injuries are the most severe and involve full-thickness tissue loss with exposed bone, tendon, or muscle. These wounds often have extensive tissue damage and can be difficult to manage. Again, non-blanchable erythema without visible skin loss is not indicative of a Stage IV pressure injury.
C. Stage II pressure injury
Stage II pressure injury Stage II pressure injuries involve partial-thickness skin loss with damage to the epidermis and possibly the dermis. These wounds often present as shallow open ulcers or blisters and may have characteristics such as intact or ruptured blisters. While Stage II injuries can present with erythema, non-blanchable erythema specifically indicates a Stage I injury.
D. Stage I pressure injury
Stage I pressure injuryStage I pressure injuries are the earliest stage and involve non-blanchable erythema of intact skin. The skin may be warmer or cooler than surrounding tissue and may have changes in sensation. There is no visible skin loss at this stage, but the area is at risk for further injury if pressure is not relieved. Therefore, non-blanchable erythema on the heels most likely indicates a Stage I pressure injury.
Full Explanation
A. Stage III pressure injury
Stage III pressure injuries involve full-thickness skin loss, extending into the subcutaneous tissue but not through the fascia. These wounds typically present as deep craters and may involve undermining or tunneling. Non-blanchable erythema alone without visible skin loss is not characteristic of a Stage III pressure injury.
B. Stage IV pressure injury
Stage IV pressure injuries are the most severe and involve full-thickness tissue loss with exposed bone, tendon, or muscle. These wounds often have extensive tissue damage and can be difficult to manage. Again, non-blanchable erythema without visible skin loss is not indicative of a Stage IV pressure injury.
C. Stage II pressure injury
Stage II pressure injuries involve partial-thickness skin loss with damage to the epidermis and possibly the dermis. These wounds often present as shallow open ulcers or blisters and may have characteristics such as intact or ruptured blisters. While Stage II injuries can present with erythema, non-blanchable erythema specifically indicates a Stage I injury.
D. Stage I pressure injury
Stage I pressure injuries are the earliest stage and involve non-blanchable erythema of intact skin. The skin may be warmer or cooler than surrounding tissue and may have changes in sensation. There is no visible skin loss at this stage, but the area is at risk for further injury if pressure is not relieved. Therefore, non-blanchable erythema on the heels most likely indicates a Stage I pressure injury.
A nurse is caring for a client who has sustained a gasoline burn to 25% of the body. Which of the following is a priority safety concern when caring for this client?
A. Elevation of the head of the bed by 30 degrees
Elevation of the head of the bed by 30 degrees: While elevation of the head of the bed may be necessary for certain medical conditions, it is not the priority concern in a client with a gasoline burn. Decontamination and assessment of the burn injury take precedence.
B. Determining the amount of gasoline that the client encountered
Determining the amount of gasoline that the client encountered: While it's important to gather information about the circumstances of the injury, including the amount of gasoline involved, this is not the priority concern at the immediate moment. Decontamination and assessment of the burn take precedence over obtaining historical information.
C. Asking the client when they last ate a meal
Asking the client when they last ate a meal: While assessing the client's nutritional status and potential need for dietary interventions is important, it is not the priority safety concern in the context of a gasoline burn. Decontamination and assessment of the burn injury are more critical at this time.
D. Decontamination of the client
Decontamination of the clientWhen a client sustains a gasoline burn, the priority safety concern is to decontaminate the client. Gasoline can cause chemical burns and can be absorbed through the skin, leading to systemic effects. Therefore, it's crucial to remove any remaining gasoline from the client's skin and clothing to prevent further absorption and minimize the risk of complications.
Full Explanation
A. Elevation of the head of the bed by 30 degrees: While elevation of the head of the bed may be necessary for certain medical conditions, it is not the priority concern in a client with a gasoline burn. Decontamination and assessment of the burn injury take precedence.
B. Determining the amount of gasoline that the client encountered: While it's important to gather information about the circumstances of the injury, including the amount of gasoline involved, this is not the priority concern at the immediate moment. Decontamination and assessment of the burn take precedence over obtaining historical information.
C. Asking the client when they last ate a meal: While assessing the client's nutritional status and potential need for dietary interventions is important, it is not the priority safety concern in the context of a gasoline burn. Decontamination and assessment of the burn injury are more critical at this time.
D. Decontamination of the client
When a client sustains a gasoline burn, the priority safety concern is to decontaminate the client. Gasoline can cause chemical burns and can be absorbed through the skin, leading to systemic effects. Therefore, it's crucial to remove any remaining gasoline from the client's skin and clothing to prevent further absorption and minimize the risk of complications.
A nurse is caring for a client with a pressure injury. Which of the following should the nurse recognize as a priority in the plan of care?
A. Keeping the wound clean and non-infected
Keeping the wound clean and non-infected: When caring for a client with a pressure injury, the priority in the plan of care is to keep the wound clean and prevent infection. This involves regular wound assessment, proper wound cleaning techniques, application of appropriate dressings, and monitoring for signs of infection such as increased redness, swelling, warmth, or drainage. Preventing infection is crucial for promoting healing and preventing complications.
B. Application of a negative pressure wound care device
Application of a negative pressure wound care device: While negative pressure wound therapy (NPWT) can be beneficial in promoting wound healing, it may not be the immediate priority unless specifically indicated by the healthcare provider based on the stage and characteristics of the pressure injury. Keeping the wound clean and preventing infection take precedence over NPWT in the initial plan of care.
C. Client education on wound prevention
Client education on wound prevention: While client education is important for preventing future pressure injuries, it is not the immediate priority when caring for an existing pressure injury. The focus initially should be on managing the current wound to promote healing and prevent complications.
D. Promoting a high carbohydrate, low protein diet
Promoting a high carbohydrate, low protein diet: Nutritional interventions are important in wound healing, but promoting a specific diet is not the immediate priority in the plan of care for a pressure injury. Providing adequate nutrition and addressing any nutritional deficiencies may be part of the overall plan, but it is secondary to keeping the wound clean and preventing infection.
Full Explanation
A. Keeping the wound clean and non-infected: When caring for a client with a pressure injury, the priority in the plan of care is to keep the wound clean and prevent infection. This involves regular wound assessment, proper wound cleaning techniques, application of appropriate dressings, and monitoring for signs of infection such as increased redness, swelling, warmth, or drainage. Preventing infection is crucial for promoting healing and preventing complications.
B. Application of a negative pressure wound care device: While negative pressure wound therapy (NPWT) can be beneficial in promoting wound healing, it may not be the immediate priority unless specifically indicated by the healthcare provider based on the stage and characteristics of the pressure injury. Keeping the wound clean and preventing infection take precedence over NPWT in the initial plan of care.
C. Client education on wound prevention: While client education is important for preventing future pressure injuries, it is not the immediate priority when caring for an existing pressure injury. The focus initially should be on managing the current wound to promote healing and prevent complications.
D. Promoting a high carbohydrate, low protein diet: Nutritional interventions are important in wound healing, but promoting a specific diet is not the immediate priority in the plan of care for a pressure injury. Providing adequate nutrition and addressing any nutritional deficiencies may be part of the overall plan, but it is secondary to keeping the wound clean and preventing infection.