Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
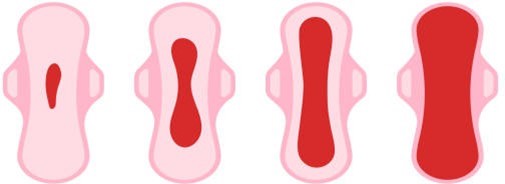
A nurse is caring for a postpartum client who saturates a perineal pad in 10 min. Which of the following actions should the nurse take first?
A. Massage the client's fundus.
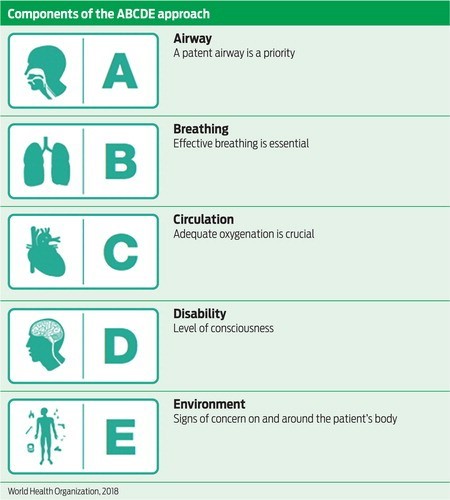
Choice A reason: Massage the client's fundus is correct, as this is the first action the nurse should take according to the ABCDE priority framework. Saturating a perineal pad in 10 min indicates excessive bleeding and possible postpartum hemorrhage, which can compromise the client's airway, breathing, and circulation. Massaging the fundus can stimulate uterine contraction and reduce blood loss.
B. Check the client's blood pressure.
Choice B reason: Check the client's blood pressure is incorrect, as this is not the first action the nurse should take, although it is important to monitor for signs of shock. Checking the blood pressure does not address the cause of bleeding or prevent further blood loss.
C. Administer oxytocin.
Choice C reason: Administer oxytocin is incorrect, as this is not the first action the nurse should take, although it may be indicated later. Administering oxytocin requires a provider's order and may have adverse effects such as nausea, vomiting, headache, or water intoxication. The nurse should first atempt to control bleeding by massaging the fundus and then administer oxytocin as ordered.
D. Observe for pooling of blood under the butocks.
Choice D reason: Observe for pooling of blood under the butocks is incorrect, as this is not the first action the nurse should take, although it can help estimate blood loss. Observing for pooling of blood does not address the cause of bleeding or prevent further blood loss. The nurse should first atempt to control bleeding by massaging the fundus and then assess for other signs of hemorrhage.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: Massage the client's fundus is correct, as this is the first action the nurse should take according to the ABCDE priority framework. Saturating a perineal pad in 10 min indicates excessive bleeding and possible postpartum hemorrhage, which can compromise the client's airway, breathing, and circulation. Massaging the fundus can stimulate uterine contraction and reduce blood loss.
Choice B reason: Check the client's blood pressure is incorrect, as this is not the first action the nurse should take, although it is important to monitor for signs of shock. Checking the blood pressure does not address the cause of bleeding or prevent further blood loss.
Choice C reason: Administer oxytocin is incorrect, as this is not the first action the nurse should take, although it may be indicated later. Administering oxytocin requires a provider's order and may have adverse effects such as nausea,
vomiting, headache, or water intoxication. The nurse should first atempt to control bleeding by massaging the fundus and then administer oxytocin as ordered.
Choice D reason: Observe for pooling of blood under the butocks is incorrect, as this is not the first action the nurse should take, although it can help estimate blood loss. Observing for pooling of blood does not address the cause of bleeding or prevent further blood loss. The nurse should first atempt to control bleeding by massaging the fundus and then assess for other signs of hemorrhage.
Similar Questions
A nurse is assisting in the care of a client who is in labor. The doctor documents the vaginal examination as: 3 cm, 30%, and -1. The nurse evaluates this documentation to mean which of the following?
A. The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm above the ischial spines.
Choice A reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm above the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
B. The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm above the ischial spines.
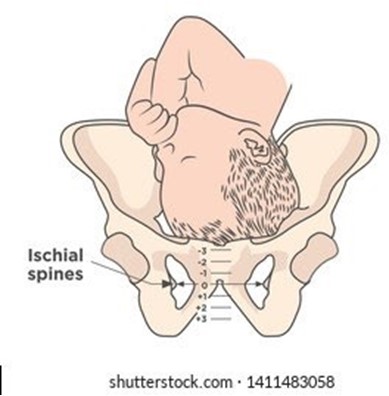
Choice B reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm above the ischial spines is correct, as this follows the correct order and measurement of cervical assessment. Cervical dilation, effacement, and station are recorded in that order to describe the progress of labor. Station refers to the relationship between the presenting part of the fetus and the maternal pelvis, measured by the level of the ischial spines. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
C. The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm below the ischial spines.
Choice C reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
D. The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm below the ischial spines.
Choice D reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not match the documentation of station. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
Full Explanation
Choice A reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm above the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
Choice B reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm above the ischial spines is correct, as this follows the correct order and measurement of cervical assessment. Cervical dilation, effacement, and station are recorded in that order to describe the progress of labor. Station refers to the relationship between the presenting part of the fetus and the maternal pelvis, measured by the level of the ischial spines. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
Choice C reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
Choice D reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not match the documentation of station. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
A nurse is caring for a client who is 4 hr postpartum. The nurse finds a small amount of lochia rubra on the client's perineal pad. The fundus is midline and firm at the umbilicus. Which of the following actions should the nurse take?
A. Perform fundal massage.
Choice A reason: Perform fundal massage is incorrect, as this action is not indicated for a client who has a firm and midline fundus. Fundal massage is used to stimulate uterine contraction and prevent hemorrhage in clients who have a boggy or deviated fundus.
B. Assist the client to ambulate.
Choice B reason: Assist the client to ambulate is correct, as this action can promote lochia drainage and prevent pooling of blood in the vagina. The nurse should encourage the client to ambulate early and frequently after birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide assistance as needed.
C. Check for blood under the client's butock.
Choice C reason: Check for blood under the client's butock is incorrect, as this action is not necessary for a client who has a small amount of lochia rubra on the perineal pad. Lochia rubra is normal and expected in the first few days after birth, and it indicates that the placental site is healing. The nurse should check for blood under the butock only if there is suspicion of excessive bleeding or concealed hemorrhage.
D. Increase the rate of the IV fluids.
Choice D reason: Increase the rate of the IV fluids is incorrect, as this action is not indicated for a client who has a small amount of lochia rubra on the perineal pad. Increasing the rate of IV fluids can cause fluid overload and electrolyte imbalance in the client. The nurse should maintain the IV fluids at the prescribed rate and monitor the client's intake and output.
Full Explanation
Choice A reason: Perform fundal massage is incorrect, as this action is not indicated for a client who has a firm and midline fundus. Fundal massage is used to stimulate uterine contraction and prevent hemorrhage in clients who have a boggy or deviated fundus.
Choice B reason: Assist the client to ambulate is correct, as this action can promote lochia drainage and prevent pooling of blood in the vagina. The nurse should encourage the client to ambulate early and frequently after birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide assistance as needed.
Choice C reason: Check for blood under the client's butock is incorrect, as this action is not necessary for a client who has a small amount of lochia rubra on the perineal pad. Lochia rubra is normal and expected in the first few days after birth, and it indicates that the placental site is healing. The nurse should check for blood under the butock only if there is suspicion of excessive bleeding or concealed hemorrhage.
Choice D reason: Increase the rate of the IV fluids is incorrect, as this action is not indicated for a client who has a small amount of lochia rubra on the perineal pad. Increasing the rate of IV fluids can cause fluid overload and electrolyte imbalance in the client. The nurse should maintain the IV fluids at the prescribed rate and monitor the client's intake and output.
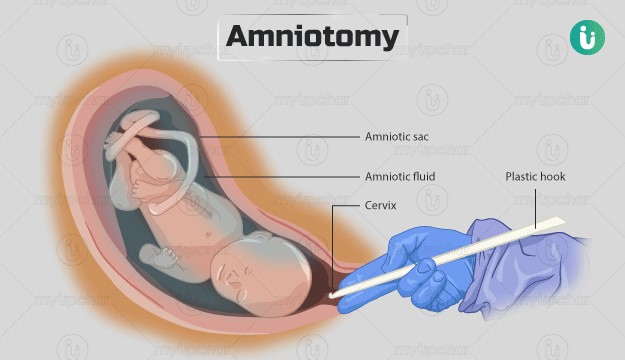
A nurse is assisting in the care of a client following an amniotomy who is now in the active phase of the first stage of labor. Which of the following actions should the nurse take?
A. Check the client's temperature every 4 hr.
Choice A reason: Check the client's temperature every 4 hr is incorrect, as this action is not frequent enough for a client who had an amniotomy. The nurse should check the client's temperature every 2 hr after an amniotomy, as there is an increased risk of infection due to the rupture of membranes. The nurse should also monitor for signs of chorioamnionitis, such as foul-smelling amniotic fluid, maternal tachycardia, or fetal tachycardia.
B. Remind the client to bear down with each contraction.
Choice B reason: Remind the client to bear down with each contraction is incorrect, as this action is not appropriate for a client who is in the active phase of the first stage of labor. The nurse should instruct the client to avoid bearing down or pushing until they are in the second stage of labor, when the cervix is fully dilated and effaced. Bearing down too early can cause cervical edema, lacerations, or exhaustion.
C. Maintain the client in the lithotomy position.
Choice C reason: Maintain the client in the lithotomy position is incorrect, as this action is not optimal for a client who is in the active phase of the first stage of labor. The lithotomy position is a supine position with the legs elevated and abducted, which can reduce blood flow to the uterus and placenta, increase perineal edema, and limit pelvic outlet diameter. The nurse should encourage the client to change positions frequently and use upright or lateral positions that can enhance uterine contractility, fetal descent, and maternal comfort.
D. Encourage the client to empty the bladder every 2 hr.
Choice D reason: Encourage the client to empty the bladder every 2 hr is correct, as this action can promote labor progress and prevent bladder distension and infection. The nurse should assist the client to void every 2 hr after an amniotomy, as there may be decreased sensation of bladder fullness due to pressure from the fetal head. A full bladder can interfere with uterine contractions, fetal descent, and cervical dilation.
Full Explanation
Choice A reason: Check the client's temperature every 4 hr is incorrect, as this action is not frequent enough for a client who had an amniotomy. The nurse should check the client's temperature every 2 hr after an amniotomy, as there is an increased risk of infection due to the rupture of membranes. The nurse should also monitor for signs of chorioamnionitis, such as foul-smelling amniotic fluid, maternal tachycardia, or fetal tachycardia.
Choice B reason: Remind the client to bear down with each contraction is incorrect, as this action is not appropriate for a client who is in the active phase of the first stage of labor. The nurse should instruct the client to avoid bearing down or pushing until they are in the second stage of labor, when the cervix is fully dilated and effaced. Bearing down too early can cause cervical edema, lacerations, or exhaustion.
Choice C reason: Maintain the client in the lithotomy position is incorrect, as this action is not optimal for a client who is in the active phase of the first stage of labor. The lithotomy position is a supine position with the legs elevated and abducted, which can reduce blood flow to the uterus and placenta, increase perineal edema, and limit pelvic outlet diameter. The nurse should encourage the client to change positions frequently and use upright or lateral positions that can enhance uterine contractility, fetal descent, and maternal comfort.
Choice D reason: Encourage the client to empty the bladder every 2 hr is correct, as this action can promote labor progress and prevent bladder distension and infection. The nurse should assist the client to void every 2 hr after an amniotomy, as there may be decreased sensation of bladder fullness due to pressure from the fetal head. A full bladder can interfere with uterine contractions, fetal descent, and cervical dilation.