Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is caring for a preschooler with a partial-thickness burn on her right forearm. Which of the following findings should the nurse expect? (Select all that apply.).
A. Intact epidermis.
Choice A is not the answer because a partial-thickness burn affects both the outer layer of skin (epidermis) and the layer beneath it (dermis), so the epidermis would not be intact.
B. Dry surface.
Choice B is not the answer because partial-thickness burns can have a moist surface due to blistering.
C. Sensitive to touch.
Partial-thickness burns can be described by redness, swelling, and blisters. The skin is usually reddened and may be sensitive to touch.
D. Wound blanches with pressure.
Wound blanches with pressure because the blood vessels are damaged, allowing blanching on pressure.
E. Blisters.
Partial-thickness burns can be described by redness, swelling, and blisters. The skin is usually reddened and may be sensitive to touch.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Custom SP23 N23 N240 Proctored Exam 3 Ch 11 24 32 43 44. Take the full exam now
Full Explanation
The correct answers are C, D, and E.
Choice A rationale: Intact epidermis would not be expected with a partial-thickness burn as the burn extends into the dermis.
Choice B rationale: A dry surface is not characteristic of partial-thickness burns, which typically have a moist surface.
Choice C rationale: Partial-thickness burns are sensitive to touch due to the damage to nerve endings in the dermis.
Choice D rationale: Wound blanches with pressure because the blood vessels are damaged, allowing blanching on pressure.
Choice E rationale: Blisters are a common feature of partial-thickness burns, as the damage to the dermis causes fluid to accumulate.
Similar Questions
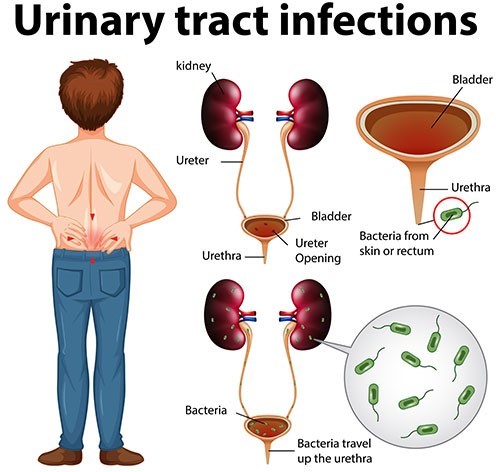
A nurse is teaching a parent of a child who has a urinary tract infection. Which of the following should the nurse include in the teaching? (Select all that apply).
A. Avoid bubble baths.
Avoiding bubble baths can help prevent irritation and infection.
B. Watch for manifestations of infection.
Watching for manifestations of infection can help detect any worsening or recurrence of the infection.
C. Empty the bladder completely with each void.
Emptying the bladder completely with each void can help prevent urine from remaining in the bladder and causing infection.
D. Wipe perineal area front to back.
Wiping the perineal area front to back can help prevent bacteria fromspreading to the urethra.
E. Wear cotton underpants.
Wearing cotton underpants can help keep the area dry and reduce the risk of infection.
Full Explanation
The nurse should include all of these points in the teaching.
A. Avoiding bubble baths can help prevent irritation and infection.
B. Watching for manifestations of infection can help detect any worsening or recurrence of the infection.
C. Emptying the bladder completely with each void can help prevent urine from remaining in the bladder and causing infection.
D. Wiping the perineal area front to back can help prevent bacteria from
spreading to the urethra.
E. Wearing cotton underpants can help keep the area dry and reduce the risk of infection.
A nurse is planning care for an adolescent who is postoperative following scoliosis repair with Harrington rod instrumentation. Which of the following interventions should the nurse include in the plan of care?
A. Reposition the client by log rolling every 4 hr.
Log rolling is an appropriate technique to reposition a postoperative scoliosis repair patient as it minimizes stress on the spine and helps maintain spinal alignment. Patients need frequent repositioning to prevent pressure ulcers and promote comfort, but every 4 hours may not be frequent enough; typically, every 2 hours is recommended.
B. Place the client in protective isolation.
b. Protective isolation is not typically required for patients undergoing scoliosis surgery unless they have specific risk factors for infection (e.g., immunocompromised status). Standard postoperative care focuses on monitoring for infection at the surgical site rather than isolation unless indicated by the patient's condition.
C. Keep the head of the bed at a 30° angle.
While it’s important to elevate the head of the bed to assist with breathing and comfort, after scoliosis surgery, the head of the bed is generally elevated to 30-45° to facilitate lung expansion and reduce the risk of aspiration. However, it should be ensured that this angle does not compromise spinal alignment, especially in the early postoperative period.
D. Initiate the use of a PCA pump for pain control.
The use of a patient-controlled analgesia (PCA) pump is an appropriate intervention for pain management after scoliosis surgery. It allows the patient to self-administer pain medication within prescribed limits, leading to more effective pain management, improved patient satisfaction, and potentially reduced need for supplemental analgesics.
Full Explanation
a. Log rolling is an appropriate technique to reposition a postoperative scoliosis repair patient as it minimizes stress on the spine and helps maintain spinal alignment. Patients need frequent repositioning to prevent pressure ulcers and promote comfort, but every 4 hours may not be frequent enough; typically, every 2 hours is recommended.
b. Protective isolation is not typically required for patients undergoing scoliosis surgery unless they have specific risk factors for infection (e.g., immunocompromised status). Standard postoperative care focuses on monitoring for infection at the surgical site rather than isolation unless indicated by the patient's condition.
c. While it’s important to elevate the head of the bed to assist with breathing and comfort, after scoliosis surgery, the head of the bed is generally elevated to 30-45° to facilitate lung expansion and reduce the risk of aspiration. However, it should be ensured that this angle does not compromise spinal alignment, especially in the early postoperative period.
d. The use of a patient-controlled analgesia (PCA) pump is an appropriate intervention for pain management after scoliosis surgery. It allows the patient to self-administer pain medication within prescribed limits, leading to more effective pain management, improved patient satisfaction, and potentially reduced need for supplemental analgesics.
A nurse participating in lead screening at a community center.
The nurse should instruct parents to bring their children back for rescreening in a year for which of the following laboratory values?
A. 10 mcg/dL
A lead level of 10 mcg/dL is above the CDC’s reference value of 3.5 mcg/dL and would require more immediate follow-up and intervention, not just rescreening in one year.
B. 18 mcg/dL
A lead level of 18 mcg/dL is significantly elevated and would necessitate immediate medical intervention and frequent monitoring, rather than waiting a year for rescreening.
C. 4 mcg/dL
A lead level of 4 mcg/dL is slightly above the CDC’s reference value of 3.5 mcg/dL. While it is concerning, it may be appropriate to rescreen in one year if no other risk factors are present.
D. 44 mcg/dL.
A lead level of 44 mcg/dL is dangerously high and requires urgent medical treatment and frequent follow-up, not just rescreening in one year.
Full Explanation
The correct answer is choice C.
Choice A rationale:
A lead level of 10 mcg/dL is above the CDC’s reference value of 3.5 mcg/dL and would require more immediate follow-up and intervention, not just rescreening in one year.
Choice B rationale:
A lead level of 18 mcg/dL is significantly elevated and would necessitate immediate medical intervention and frequent monitoring, rather than waiting a year for rescreening.
Choice C rationale:
A lead level of 4 mcg/dL is slightly above the CDC’s reference value of 3.5 mcg/dL. While it is concerning, it may be appropriate to rescreen in one year if no other risk factors are present.
Choice D rationale:
A lead level of 44 mcg/dL is dangerously high and requires urgent medical treatment and frequent follow-up, not just rescreening in one year.