Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
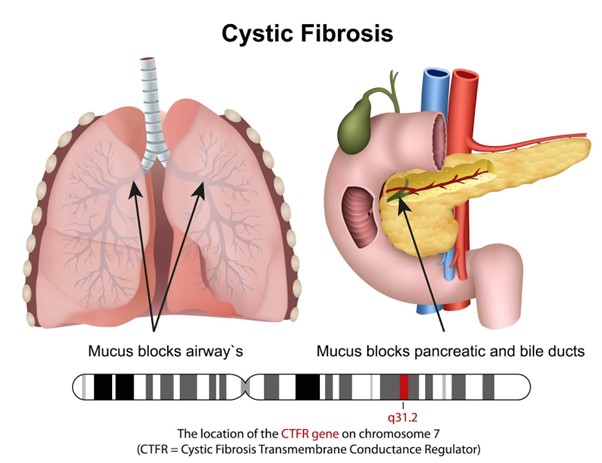
A nurse is caring for an adolescent client who has cystic fibrosis. Which of the following actions should the nurse instruct the client to take prior to initiating postural drainage?
A. Complete oral hygiene.
Completing oral hygiene is important for overall health, especially for individuals with cystic fibrosis, as they are at a higher risk for dental problems due to thick mucus that can harbor bacteria. However, oral hygiene does not have a direct impact on the effectiveness of postural drainage. Postural drainage is a technique used to clear mucus from the lungs, and while maintaining oral hygiene is beneficial, it is not a prerequisite for this procedure.
B. Use an ibuterol inhaler.
Using a bronchodilator, such as an ibuterol inhaler, is recommended before postural drainage because it helps to open the airways, making the procedure more effective. Bronchodilators work by relaxing the muscles around the airways, which can become constricted in conditions like cystic fibrosis. This relaxation allows for easier clearance of mucus during postural drainage.
C. Take pancrelipase.
Pancrelipase is an enzyme supplement used to aid digestion in patients with cystic fibrosis, who often have pancreatic insufficiency. While taking pancrelipase is crucial for nutrient absorption, it is not specifically related to the respiratory treatment of postural drainage. Therefore, it is not necessary to take pancrelipase immediately before this procedure.
D. Eat a meal.
Eating a meal before postural drainage is not recommended. The procedure involves placing the body in positions that facilitate the drainage of mucus from the lungs due to gravity. Having a full stomach can cause discomfort, increase the risk of vomiting, and may hinder the effectiveness of the drainage. It is best to perform postural drainage when the stomach is empty, either before meals or at least 1.5 hours after eating.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Comprehensive Predictor 2023 Exit Proctored Exam A. Take the full exam now
Full Explanation
The correct answer is B.
Choice A reason: Completing oral hygiene is important for overall health, especially for individuals with cystic fibrosis, as they are at a higher risk for dental problems due to thick mucus that can harbor bacteria. However, oral hygiene does not have a direct impact on the effectiveness of postural drainage. Postural drainage is a technique used to clear mucus from the lungs, and while maintaining oral hygiene is beneficial, it is not a prerequisite for this procedure.
Choice B reason: Using a bronchodilator, such as an ibuterol inhaler, is recommended before postural drainage because it helps to open the airways, making the procedure more effective. Bronchodilators work by relaxing the muscles around the airways, which can become constricted in conditions like cystic fibrosis. This relaxation allows for easier clearance of mucus during postural drainage.
Choice C reason: Pancrelipase is an enzyme supplement used to aid digestion in patients with cystic fibrosis, who often have pancreatic insufficiency. While taking pancrelipase is crucial for nutrient absorption, it is not specifically related to the respiratory treatment of postural drainage. Therefore, it is not necessary to take pancrelipase immediately before this procedure.
Choice D reason: Eating a meal before postural drainage is not recommended. The procedure involves placing the body in positions that facilitate the drainage of mucus from the lungs due to gravity. Having a full stomach can cause discomfort, increase the risk of vomiting, and may hinder the effectiveness of the drainage. It is best to perform postural drainage when the stomach is empty, either before meals or at least 1.5 hours after eating.
Similar Questions
A nurse is providing teaching to a client who is to begin external radiation therapy for cancer. Which of the following information should the nurse include?
A. "You might experience altered taste sensations."
"You might experience altered taste sensations" is the correct statement. When providing teaching to a client about to undergo external radiation therapy for cancer, the nurse should include information about potential side effects and what to expect during the treatment. One common side effect of radiation therapy, especially when the treatment is focused on or near the head and neck region, is altered taste sensations. Radiation can affect the taste buds and lead to changes in how foods taste.
B. "Use rubbing alcohol to remove the ink markings."
"Use rubbing alcohol to remove the ink markings. “The statement is incorrect. The ink markings made on the client's skin are used as reference points for the radiation therapy treatment. It is essential not to remove these markings, as they are crucial for accurate positioning during each treatment session. The nurse should instruct the client not to tamper with the markings, and the radiation therapy team will remove them when they are no longer needed.
C. "Wear a binder over the radiation site."
"Wear a binder over the radiation site." The statement is incorrect. Wearing a binder over the radiation site is not a standard practice during external radiation therapy. The client should be instructed to follow the specific guidelines provided by the radiation therapy team regarding clothing and positioning during treatments. The use of binders or other tight clothing over the treatment area may not be recommended, as it can cause discomfort or interfere with the delivery of radiation.
D. "Wash your skin thoroughly with a washcloth after each treatment."
"Wash your skin thoroughly with a washcloth after each treatment." Is incorrect statement. During radiation therapy, the skin in the treatment area can become sensitive. It is essential for the client to follow the specific instructions provided by the radiation therapy team regarding skin care. Generally, the client should avoid using harsh soaps or scrubbing the skin vigorously. Instead, they should gently cleanse the area with a mild soap or as directed by their healthcare providers.
Full Explanation
Choice A reason:
"You might experience altered taste sensations" is the correct statement. When providing teaching to a client about to undergo external radiation therapy for cancer, the nurse should include information about potential side effects and what to expect during the treatment. One common side effect of radiation therapy, especially when the treatment is focused on or near the head and neck region, is altered taste sensations. Radiation can affect the taste buds and lead to changes in how foods taste.
Choice B reason:
"Use rubbing alcohol to remove the ink markings. “The statement is incorrect. The ink markings made on the client's skin are used as reference points for the radiation therapy treatment. It is essential not to remove these markings, as they are crucial for accurate positioning during each treatment session. The nurse should instruct the client not to tamper with the markings, and the radiation therapy team will remove them when they are no longer needed.
Choice C reason:
"Wear a binder over the radiation site." The statement is incorrect. Wearing a binder over the radiation site is not a standard practice during external radiation therapy. The client should be instructed to follow the specific guidelines provided by the radiation therapy team regarding clothing and positioning during treatments. The use of binders or other tight clothing over the treatment area may not be recommended, as it can cause discomfort or interfere with the delivery of radiation.
Choice D reason
"Wash your skin thoroughly with a washcloth after each treatment." Is incorrect statement. During radiation therapy, the skin in the treatment area can become sensitive. It is essential for the client to follow the specific instructions provided by the radiation therapy team regarding skin care. Generally, the client should avoid using harsh soaps or scrubbing the skin vigorously. Instead, they should gently cleanse the area with a mild soap or as directed by their healthcare providers.

A nurse is providing teaching to an older adult client who has a seizure disorder and a new prescription for phenytoin. Which of the following instructions should the nurse include?
A. "Plan to take this medication with food."
"Plan to take this medication with food." Is the correct statement. When providing instructions to an older adult client who has a seizure disorder and is prescribed phenytoin (an antiepileptic or anticonvulsant medication), the nurse should advise the client to take the medication with food. Phenytoin can cause gastrointestinal irritation, and taking it with food can help minimize this side effect.
B. "Plan to take this medication with antacids."
"Plan to take this medication with antacids. “is not the appropriate instruction. Phenytoin should not be taken with antacids. Antacids can reduce the absorption of phenytoin, leading to decreased effectiveness of the medication. If antacids are needed for other reasons, they should be taken at least 2 hours before or after taking phenytoin.
C. "Limit foods that contain vitamin D while taking this medication."
"Limit foods that contain vitamin D while taking this medication. “This is not inappropriate instruction. There is no specific requirement to limit foods containing vitamin D while taking phenytoin. However, phenytoin may decrease the absorption of vitamin D, which could potentially affect the client's vitamin D levels. Therefore, it is essential for the client to have regular check-ups and possibly discuss the need for vitamin D supplementation with their healthcare provider.
D. "Limit foods that contain folic acid while taking this medication."
"Limit foods that contain folic acid while taking this medication. “This is not the correct statement. Phenytoin can interfere with the absorption of folic acid (a B-vitamin). Long-term use of phenytoin may lead to folic acid deficiency. Therefore, the nurse should instruct the client to consume foods rich in folic acid and discuss the potential need for folic acid supplementation with their healthcare provider.
Full Explanation
Choice A reason:
"Plan to take this medication with food." Is the correct statement. When providing instructions to an older adult client who has a seizure disorder and is prescribed phenytoin (an antiepileptic or anticonvulsant medication), the nurse should advise the client to take the medication with food. Phenytoin can cause gastrointestinal irritation, and taking it with food can help minimize this side effect.
Choice B reason:
"Plan to take this medication with antacids. “is not the appropriate instruction. Phenytoin should not be taken with antacids. Antacids can reduce the absorption of phenytoin, leading to decreased effectiveness of the medication. If antacids are needed for other reasons, they should be taken at least 2 hours before or after taking phenytoin.
Choice C reason:
"Limit foods that contain vitamin D while taking this medication. “This is not inappropriate instruction. There is no specific requirement to limit foods containing vitamin D while taking phenytoin. However, phenytoin may decrease the absorption of vitamin D, which could potentially affect the client's vitamin D levels. Therefore, it is essential for the client to have regular check-ups and possibly discuss the need for vitamin D supplementation with their healthcare provider.
Choice D reason:
"Limit foods that contain folic acid while taking this medication. “This is not the correct statement. Phenytoin can interfere with the absorption of folic acid (a B-vitamin). Long-term use of phenytoin may lead to folic acid deficiency. Therefore, the nurse should instruct the client to consume foods rich in folic acid and discuss the potential need for folic acid supplementation with their healthcare provider.
A nurse is caring for a client who received 50,000 units of IV heparin rather than the prescribed 5,000 units. Which of the following actions should the nurse take first?
A. Complete an incident report.
Completing an incident report is not the correct action. An incident report should be completed as part of the hospital's protocol to document the medication error and ensure appropriate follow-up and investigation.
B. Check the client for indications of bleeding.
Checking the client for indications of bleeding is the correct action to be taken. In this situation, the nurse's first priority should be to assess the client for indications of bleeding, as the client received a significantly higher dose of IV heparin than prescribed. Heparin is an anticoagulant medication used to prevent blood clots, and an overdose can increase the risk of bleeding. After administering the wrong dose of medication, the nurse's immediate concern is the client's safety and well-being. Checking for signs of bleeding, such as petechiae, ecchymosis, hematomas, bleeding gums, melena (black, tarry stools), haematuria (blood in urine), or any other unusual bleeding, is crucial.
C. Monitor the client's aPTT levels
Monitor the client's aPTT levels: This is not the correct action to be taken. Monitoring the client's activated partial thromboplastin time (aPTT) levels is essential to assess the client's coagulation status and determine if the overdose of heparin has affected their clotting ability. The healthcare provider may adjust the heparin dosage based on the aPTT levels.
D. Notify the risk manager.
Notify the risk manager: This is not the correct action to be taken. The risk manager or appropriate supervisor should be informed about the medication error as soon as possible to initiate a thorough review of the incident and take necessary steps to prevent similar errors in the future.
Full Explanation
Choice A reason:
Completing an incident report is not the correct action. An incident report should be completed as part of the hospital's protocol to document the medication error and ensure appropriate follow-up and investigation.
Choice B reason:
Checking the client for indications of bleeding is the correct action to be taken. In this situation, the nurse's first priority should be to assess the client for indications of bleeding, as the client received a significantly higher dose of IV heparin than prescribed. Heparin is an anticoagulant medication used to prevent blood clots, and an overdose can increase the risk of bleeding.
After administering the wrong dose of medication, the nurse's immediate concern is the client's safety and well-being. Checking for signs of bleeding, such as petechiae, ecchymosis, hematomas, bleeding gums, melena (black, tarry stools), haematuria (blood in urine), or any other unusual bleeding, is crucial.
Choice C reason:
Monitor the client's aPTT levels: This is not the correct action to be taken. Monitoring the client's activated partial thromboplastin time (aPTT) levels is essential to assess the client's coagulation status and determine if the overdose of heparin has affected their clotting ability. The healthcare provider may adjust the heparin dosage based on the aPTT levels.
Choice D reason:
Notify the risk manager: This is not the correct action to be taken. The risk manager or appropriate supervisor should be informed about the medication error as soon as possible to initiate a thorough review of the incident and take necessary steps to prevent similar errors in the future.