Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is collecting data for a client who is receiving enteral tube feedings. The nurse should identify that which of the following findings is a manifestation of fluid overload?
A. Weight loss
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
B. Decreased blood pressure
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
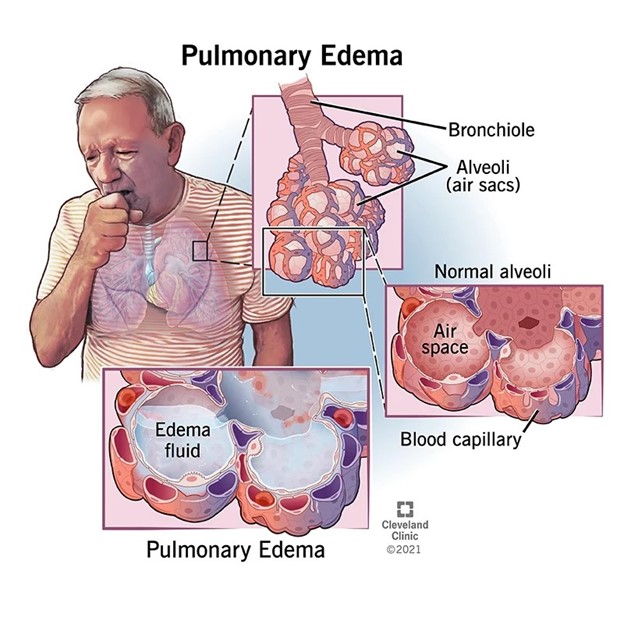
C. Crackles heard in the lungs
Fluid overload refers to an excess volume of fluid in the body, which can occur as a result of various factors, including excessive fluid intake or inadequate fluid removal. Crackles heard in the lungs, also known as rales, can indicate fluid accumulation in the lungs, a condition known as pulmonary edema. It is a common manifestation of fluid overload and can be detected through auscultation of the lungs.
D. Decreased skin turgor
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
This question is an excerpt from Nurse Dive's nursing test bank - ATI PN Comprehensive Predictor 2023 - Proctored Exam 1. Take the full exam now
Full Explanation
Fluid overload refers to an excess volume of fluid in the body, which can occur as a result of various factors, including excessive fluid intake or inadequate fluid removal. Crackles heard in the lungs, also known as rales, can indicate fluid accumulation in the lungs, a condition known as pulmonary edema. It is a common manifestation of fluid overload and can be detected through auscultation of the lungs.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Similar Questions
A nurse is performing nasopharyngeal suctioning for an adult client. Which of the following techniques should the nurse use?
A. Apply suction while inserting the catheter.
This is incorrect because suction should not be applied during the insertion of the catheter. Suctioning should only be applied while withdrawing the catheter to avoid causing trauma to the mucosa.
B. Apply intermittent suction for 15 seconds.
Suctioning should generally be performed for no longer than 10 seconds at a time to minimize the risk of complications such as hypoxia.
C. Wait 1 min between suctioning attempts.
This response is correct because waiting approximately 1 minute between suctioning attempts allows the client time to recover and reoxygenate. This interval helps prevent hypoxia and mucosal damage, which are important considerations during the suctioning process.
D. Insert the catheter 10 cm (4 in).
In adults insert catheter approximately 16 cm (6.5 inches); in older children, 8– 12 cm (3–5 inches); in infants and young children, 4–7.5 cm (1.5–3 inches). Rule of thumb is to insert catheter distance from tip of nose (or mouth) to angle of mandible.
Full Explanation
A. This is incorrect because suction should not be applied during the insertion of the catheter. Suctioning should only be applied while withdrawing the catheter to avoid causing trauma to the mucosa.
B. Suctioning should generally be performed for no longer than 10 seconds at a time to minimize the risk of complications such as hypoxia.
C. This response is correct because waiting approximately 1 minute between suctioning attempts allows the client time to recover and reoxygenate. This interval helps prevent hypoxia and mucosal damage, which are important considerations during the suctioning process.
D. In adults insert catheter approximately 16 cm (6.5 inches); in older children, 8– 12 cm (3–5 inches); in infants and young children, 4–7.5 cm (1.5–3 inches). Rule of thumb is to insert catheter distance from tip of nose (or mouth) to angle of mandible.
A nurse is caring for a preschooler who recently experienced the death of a parent. Which of the following findings should the nurse identify as consistent with this age group?
A. Believes the death is punishment for bad behavior
Preschool-aged children (typically 3 to 5 years old) often have magical thinking and may believe that their thoughts or actions can cause events to happen. They may think that the death of a parent is a punishment for something they did or thought, reflecting their egocentric view of the world.
B. Recognizes the parent will never wake up
This understanding is more commonly seen in older children who have a more mature grasp of death. Preschool-aged children may not fully comprehend that death is irreversible and permanent.
C. Expresses curiosity about the funeral service
While preschoolers might ask questions about the funeral out of curiosity, this is not the primary way they process or react to the death of a loved one. Their questions are often more about trying to understand what is happening rather than a genuine curiosity about the specifics of the service.
D. Understands that everyone dies eventually
While preschool-aged children may have some understanding that death is a natural part of life, their comprehension of its full implications is limited. They may not fully grasp the universality of death and its inevitability for all living beings
Full Explanation
Correct answer: A
Preschool-aged children (around 3 to 5 years old) have a limited understanding of death compared to older children or adults. They may not fully grasp the finality and permanence of death. They often have a more concrete and literal understanding of death.
A. Believing the death is punishment for bad behavior: Preschool-aged children (typically 3 to 5 years old) often have magical thinking and may believe that their thoughts or actions can cause events to happen. They may think that the death of a parent is a punishment for something they did or thought, reflecting their egocentric view of the world.
B. Recognizing the parent will never wake up: This understanding is more commonly seen in older children who have a more mature grasp of death. Preschool-aged children may not fully comprehend that death is irreversible and permanent.
C. While preschoolers might ask questions about the funeral out of curiosity, this is not the primary way they process or react to the death of a loved one. Their questions are often more about trying to understand what is happening rather than a genuine curiosity about the specifics of the service.
D. Understanding that everyone dies eventually: While preschool-aged children may have some understanding that death is a natural part of life, their comprehension of its full implications is limited. They may not fully grasp the universality of death and its inevitability for all living beings.
A nurse is caring for a client who speaks a different language than the nurse.
Which of the following actions should the nurse take?
A. Supplement spoken language with pictures.
Using visual aids such as pictures, diagrams, or translation cards can help bridge the communication gap between the nurse and the client. This approach ensures better understanding and reduces miscommunication, especially when discussing procedures, medications, or discharge instructions.
B. Ask a family member of the client to interpret.
This is not appropriate because family members may misinterpret medical information, omit details, or add their own opinions. A trained medical interpreter should be used to ensure accurate and confidential communication.
C. Speak to the client at an increased volume.
Is not an effective solution for a language barrier. Simply speaking louder will not address the issue of language comprehension. It is important to use appropriate communication strategies, such as seeking a qualified interpreter or using visual aids or gestures to facilitate understanding.
D. Recognize that the client nodding indicates an understanding of the information.
Nodding can have different cultural interpretations and may not always indicate comprehension. It is important to use other means of communication to confirm understanding, such as using a professional interpreter or utilizing visual aids.
Full Explanation
A. Using visual aids such as pictures, diagrams, or translation cards can help bridge the communication gap between the nurse and the client. This approach ensures better understanding and reduces miscommunication, especially when discussing procedures, medications, or discharge instructions.
B. This is not appropriate because family members may misinterpret medical information, omit details, or add their own opinions. A trained medical interpreter should be used to ensure accurate and confidential communication.
C. Speaking to the client at an increased volume in is not an effective solution for a language barrier. Simply speaking louder will not address the issue of language comprehension. It is important to use appropriate communication strategies, such as seeking a qualified interpreter or using visual aids or gestures to facilitate understanding.
D. Assuming that the client nodding indicates an understanding of the information in is not reliable. Nodding can have different cultural interpretations and may not always indicate comprehension. It is important to use other means of communication to confirm understanding, such as using a professional interpreter or utilizing visual aids.