Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
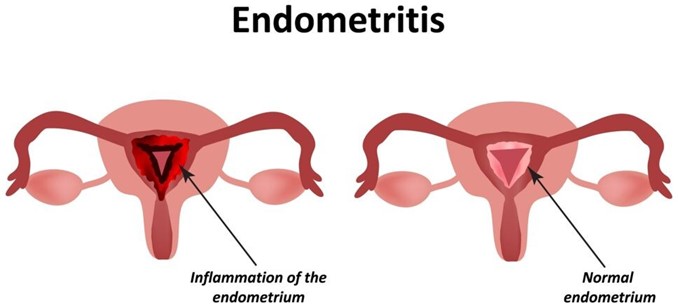
A nurse is collecting data from a client who gave birth one week ago. Which of the following findings should the nurse identify as a manifestation of endometritis?
A. Hematuria
Choice A reason: Hematuria is blood in the urine. It is not a symptom of endometritis, which is an inflammation or infection of the uterine lining. Hematuria can have many other causes, such as urinary tract infections, kidney stones, bladder cancer, or trauma.
B. Pelvic pain
Choice B reason: Pelvic pain is one of the most common symptoms of endometritis. It can be caused by the inflammation or infection of the uterine lining, which can also spread to other pelvic organs. Pelvic pain can be dull, sharp, cramping, or constant, and it may worsen with movement or intercourse¹³.
C. Pink lochia
Choice C reason: Pink lochia is normal vaginal discharge after childbirth. It consists of blood, mucus, and tissue from the uterus. It usually lasts for a few weeks and gradually changes color from red to pink to brown to white. Pink lochia is not a sign of endometritis, unless it is foul-smelling, heavy, or persists beyond six weeks.
D. Bradycardia
Choice D reason: Bradycardia is a slow heart rate, usually below 60 beats per minute. It is not a symptom of endometritis, which can cause fever and tachycardia (fast heart rate). Bradycardia can have many other causes, such as heart disease, medication side effects, hypothyroidism, or electrolyte imbalance.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Maternity Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: Hematuria is blood in the urine. It is not a symptom of endometritis, which is an inflammation or infection of the uterine lining. Hematuria can have many other causes, such as urinary tract infections, kidney stones, bladder cancer, or trauma.
Choice B reason: Pelvic pain is one of the most common symptoms of endometritis. It can be caused by the inflammation or infection of the uterine lining, which can also spread to other pelvic organs. Pelvic pain can be dull, sharp, cramping, or constant, and it may worsen with movement or intercourse¹³.
Choice C reason: Pink lochia is normal vaginal discharge after childbirth. It consists of blood, mucus, and tissue from the uterus. It usually lasts for a few weeks and gradually changes color from red to pink to brown to white. Pink lochia is not a sign of endometritis, unless it is foul-smelling, heavy, or persists beyond six weeks.
Choice D reason: Bradycardia is a slow heart rate, usually below 60 beats per minute. It is not a symptom of endometritis, which can cause fever and tachycardia (fast heart rate). Bradycardia can have many other causes, such as heart disease, medication side effects, hypothyroidism, or electrolyte imbalance.
Similar Questions
A nurse is assisting a nurse midwife in examining a client who is a primigravida at 42 weeks of gestation and states that she thinks she is in labor. Which of the following findings confirm that the client is in labor?
A. Amniotic fluid in the vaginal vault
Choice A reason: Amniotic fluid in the vaginal vault indicates that the membranes have ruptured, but this does not necessarily mean that the client is in labor. Some women may have a slow leak of amniotic fluid for hours or days before labor begins. Rupture of membranes also increases the risk of infection, so the nurse should monitor the client's temperature and fetal heart rate.
B. Contractions every 3 to 4 minutes
Choice B reason: Contractions every 3 to 4 minutes are a sign of labor, but they are not enough to confirm it. The nurse should also assess the duration and intensity of the contractions, as well as the client's response to them. Some women may have false labor contractions, also known as Braxton Hicks contractions, which are irregular, mild, and do not cause cervical changes.
C. Pain just above the navel
Choice C reason: Pain just above the navel is not a typical sign of labor. It may indicate other problems, such as placental abruption, uterine rupture, or fetal distress. The nurse should report this finding to the nurse midwife and check for other signs of bleeding, shock, or fetal compromise.
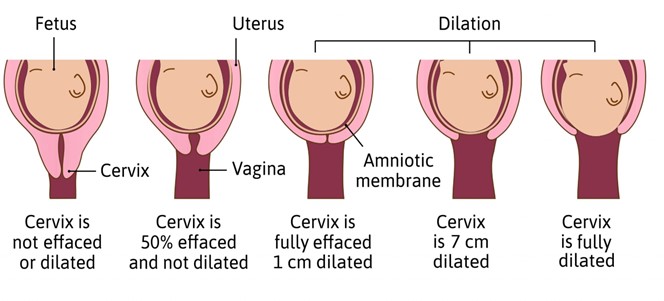
D. Cervical dilation
Choice D reason: Cervical dilation is the most reliable indicator of labor. It means that the cervix is opening and thinning out to allow the passage of the fetus. The nurse should measure the cervical dilation in centimeters and document it along with the station and effacement of the cervix.
Full Explanation
Choice A reason: Amniotic fluid in the vaginal vault indicates that the membranes have ruptured, but this does not necessarily mean that the client is in labor. Some women may have a slow leak of amniotic fluid for hours or days before labor begins. Rupture of membranes also increases the risk of infection, so the nurse should monitor the client's temperature and fetal heart rate.
Choice B reason: Contractions every 3 to 4 minutes are a sign of labor, but they are not enough to confirm it. The nurse should also assess the duration and intensity of the contractions, as well as the client's response to them. Some women may have false labor contractions, also known as Braxton Hicks contractions, which are irregular, mild, and do not cause cervical changes.
Choice C reason: Pain just above the navel is not a typical sign of labor. It may indicate other problems, such as placental abruption, uterine rupture, or fetal distress. The nurse should report this finding to the nurse midwife and check for other signs of bleeding, shock, or fetal compromise.
Choice D reason: Cervical dilation is the most reliable indicator of labor. It means that the cervix is opening and thinning out to allow the passage of the fetus. The nurse should measure the cervical dilation in centimeters and document it along with the station and effacement of the cervix.
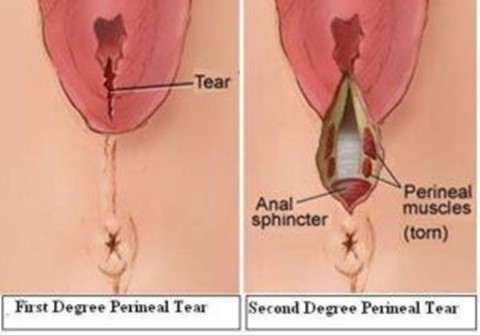
A nurse is reinforcing teaching about reducing the risk of perineal infection with a client who had a vaginal birth. Which of the following information should the nurse include in the teaching? (Select all that apply.)
A. Apply ice packs to the perineal area several times daily.
Choice A reason: While ice packs can help reduce swelling and discomfort, they are not essential for preventing infection.
B. Sit on an inflatable donut to protect the perineum.
Choice B reason: Sit on an inflatable donut to protect the perineum is incorrect, as this can increase pressure and blood flow to the perineum and delay healing. The nurse should advise the client to avoid sitting on hard or uneven surfaces and to use a pillow or a cushion for comfort.
C. Perform hand hygiene before and after voiding.
Choice C reason: Perform hand hygiene before and after voiding is correct, as this can prevent contamination and infection of the perineal area. The nurse should instruct the client to wash their hands with soap and water or use an alcohol-based hand sanitizer before and after using the toilet.
D. Blot the perineal area dry after voiding.
Choice D reason: Blot the perineal area dry after voiding is correct, as this can keep the perineal area clean and dry and prevent irritation and infection. The nurse should instruct the client to use a clean, soft cloth or tissue and gently pat or blot the perineal area from front to back after voiding.
E. Clean the perineal area from front to back.
Choice E reason: Clean the perineal area from front to back is correct, as this can prevent bacteria from entering the vagina or urethra and causing infection. The nurse should instruct the client to use a peri-botle filled with warm water and squirt it over the perineal area from front to back after each voiding or bowel movement. The client should also change their perineal pad frequently and dispose of it properly.
Full Explanation
Choice A reason: While ice packs can help reduce swelling and discomfort, they are not essential for preventing infection.
Choice B reason: Sit on an inflatable donut to protect the perineum is incorrect, as this can increase pressure and blood flow to the perineum and delay healing. The nurse should advise the client to avoid sitting on hard or uneven surfaces and to use a pillow or a cushion for comfort.
Choice C reason: Perform hand hygiene before and after voiding is correct, as this can prevent contamination and infection of the perineal area. The nurse should instruct the client to wash their hands with soap and water or use an alcohol-based hand sanitizer before and after using the toilet.
Choice D reason: Blot the perineal area dry after voiding is correct, as this can keep the perineal area clean and dry and prevent irritation and infection. The nurse should instruct the client to use a clean, soft cloth or tissue and gently pat or blot the perineal area from front to back after voiding.
Choice E reason: Clean the perineal area from front to back is correct, as this can prevent bacteria from entering the vagina or urethra and causing infection. The nurse should instruct the client to use a peri-botle filled with warm water and squirt it over the perineal area from front to back after each voiding or bowel movement. The client should also change their perineal pad frequently and dispose of it properly.
A nurse is assisting in the care of a client who had a vaginal birth 2 hr ago. Which of the following actions should the nurse take? (Select all that apply.)
A. Administer terbutaline if the fundus is boggy.
Choice A reason: Administer terbutaline if the fundus is boggy is incorrect, as this action is contraindicated for a client who has a boggy fundus. Terbutaline is a tocolytic agent that can relax uterine contractions and worsen uterine atony and hemorrhage. The nurse should administer oxytocin or other uterotonic agents as prescribed to stimulate uterine contraction and prevent bleeding.
B. Observe the lochia during palpation of fundus.
Choice B reason: Observe the lochia during palpation of fundus is correct, as this action can provide information about the amount, color, consistency, and odor of lochia. Lochia is the vaginal discharge that occurs after birth, which consists of blood, mucus, and tissue. The nurse should observe the lochia during fundal palpation and report any abnormal findings, such as excessive bleeding, large clots, foul smell, or infection.
C. Document fundal height.
Choice C reason: Document fundal height is correct, as this action can provide information about the progress of uterine involution. The fundus is the upper part of the uterus that can be palpated through the abdomen after birth. The nurse should document the fundal height in relation to the umbilicus and note any changes over time.
D. Massage a firm fundus.
Choice D reason: Massage a firm fundus is incorrect, as this action is not necessary for a client who has a firm fundus. A firm fundus indicates adequate uterine contraction and involution and prevents excessive bleeding. The nurse should massage a boggy or soft fundus until it becomes firm and midline.
E. Determine whether the fundus is midline.
Choice E reason: Determine whether the fundus is midline is correct, as this action can provide information about the position of the uterus and bladder. The fundus should be midline and not displaced to either side. A deviated fundus can indicate bladder distension, which can interfere with uterine contraction and involution and increase the risk of hemorrhage and infection. The nurse should assist the client to empty their bladder and reassess the fundal position.
Full Explanation
Choice A reason: Administer terbutaline if the fundus is boggy is incorrect, as this action is contraindicated for a client who has a boggy fundus. Terbutaline is a tocolytic agent that can relax uterine contractions and worsen uterine atony and hemorrhage. The nurse should administer oxytocin or other uterotonic agents as prescribed to stimulate uterine contraction and prevent bleeding.
Choice B reason: Observe the lochia during palpation of fundus is correct, as this action can provide information about the amount, color, consistency, and odor of lochia. Lochia is the vaginal discharge that occurs after birth, which consists of blood, mucus, and tissue. The nurse should observe the lochia during fundal palpation and report any abnormal findings, such as excessive bleeding, large clots, foul smell, or infection.
Choice C reason: Document fundal height is correct, as this action can provide information about the progress of uterine involution. The fundus is the upper part of the uterus that can be palpated through the abdomen after birth. The nurse should document the fundal height in relation to the umbilicus and note any changes over time.
Choice D reason: Massage a firm fundus is incorrect, as this action is not necessary for a client who has a firm fundus. A firm fundus indicates adequate uterine contraction and involution and prevents excessive bleeding. The nurse should massage a boggy or soft fundus until it becomes firm and midline.
Choice E reason: Determine whether the fundus is midline is correct, as this action can provide information about the position of the uterus and bladder. The fundus should be midline and not displaced to either side. A deviated fundus can indicate bladder distension, which can interfere with uterine contraction and involution and increase the risk of hemorrhage and infection. The nurse should assist the client to empty their bladder and reassess the fundal position.