Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is collecting data from a client who has a long leg cast on his left leg. Which of the following findings is the priority?
A. Ecchymosis on the inner left thigh
May be a concerning finding, but it is not as urgent as diminished pulses. Ecchymosis may be a result of trauma during cast application, and may resolve on its own.
B. One fingerbreadth of space between the cast and the skin
Is a normal finding and indicates that the cast is not too tight.
C. Diminished pulses on the affected extremity
This finding may indicate compromised circulation, which is a serious complication that requires immediate intervention.
D. Client report of muscle spasms of the left leg
Is a common complaint in clients with casts and may be addressed with medication or other interventions, but it is not as urgent as diminished pulses.
This question is an excerpt from Nurse Dive's nursing test bank - PN Comprehensive Predictor PN 2020 Proctored Exam. Take the full exam now
Full Explanation
c. Diminished pulses on the affected extremity. This finding may indicate compromised circulation, which is
a serious complication that requires immediate intervention.
Option a. Ecchymosis on the inner left thigh may be a concerning finding, but it is not as urgent as diminished pulses. Ecchymosis may be a result of trauma during cast application, and may resolve on its own.
Option b. One fingerbreadth of space between the cast and the skin is a normal finding and indicates that the cast is not too tight.
Option d. Client report of muscle spasms of the left leg is a common complaint in clients with casts and may
be addressed with medication or other interventions, but it is not as urgent as diminished pulses. Therefore, the priority finding in this scenario is c. Diminished pulses on the affected extremity.

Similar Questions
A nurse is caring for a client who has a prescription for warfarin. Which of the following laboratory tests should the nurse monitor?
A. Triiodothyronine
Is a thyroid hormone and is not directly related to warfarin therapy.
B. Blood urea nitrogen
Is a measure of kidney function and is also not directly related to warfarin therapy.
C. Arterial blood gases
Is a measure of oxygen and carbon dioxide levels in the blood and is not related to warfarin therapy.
D. Prothrombin time
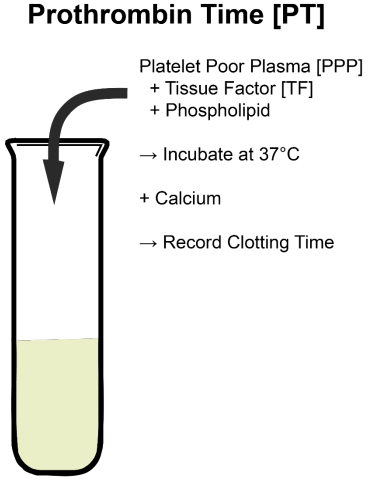
Warfarin is an anticoagulant medication that works by inhibiting the synthesis of vitamin K-dependent clotting factors in the liver. Therefore, it is important to monitor the client's clotting ability to ensure that the medication is working properly and not causing any adverse effects. The laboratory test that is used to monitor warfarin therapy is the prothrombin time (PT), which measures the time it takes for the blood to clot. The nurse should monitor the client's PT regularly and adjust the dosage of warfarin as necessary to maintain the therapeutic range.
Full Explanation
Prothrombin time.
Explanation:
When a client is prescribed warfarin, monitoring the prothrombin time (PT) and the International Normalized Ratio (INR) is crucial. Warfarin is an anticoagulant medication that affects the clotting ability of the blood by inhibiting vitamin K-dependent clotting factors. Monitoring the prothrombin time and INR helps determine the client's blood's ability to clot and the appropriate dosage of warfarin to maintain the desired therapeutic range.
Option a (Triiodothyronine) is a thyroid hormone and is not directly related to warfarin therapy.
Option b (Blood urea nitrogen) is a measure of kidney function and is also not directly related to warfarin therapy.
Option c (Arterial blood gases) is a measure of oxygen and carbon dioxide levels in the blood and is not related to warfarin therapy.
A nurse is assisting with the care of a client.
Complete the following sentence.
After notifying the provider, the nurse should first and then . (Separate your answers with a comma ',')
Full Explanation
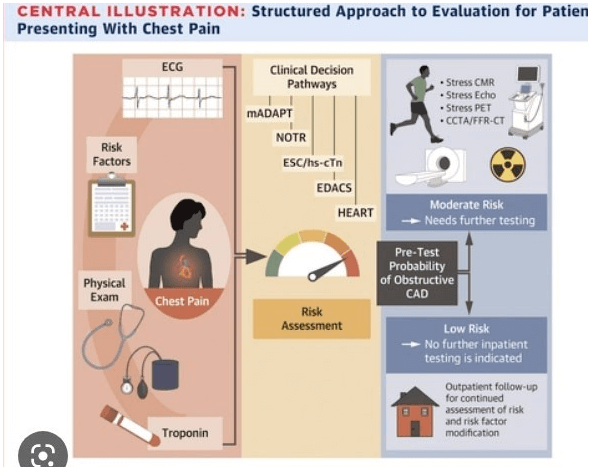
The client's symptoms are concerning for angina or a possible myocardial infarction (heart atack) and require immediate intervention. Nitroglycerin is a medication that can help relieve chest pain associated with cardiac events by dilating blood vessels and reducing the workload on the heart.
Therefore, the nurse should administer nitroglycerin as ordered by the provider. After administering nitroglycerin, the nurse should obtain an ECG to assess for any changes in cardiac rhythm or evidence of ischemia (lack of blood flow to the heart muscle).
The ECG can provide important diagnostic information and guide further treatment decisions.
A nurse is assisting with the care of a client.
Laboratory Results
Abdominal ultrasound: mass present in small intestine proximal to ileocecal valve. Size of mass is 6 cm x 7 cm (2.4 in x 2.8 in).
Select the 4 responsibilities the nurse has in relation to the client's advance directives.
A. Inform the client that an advance directive discontinues further care.
An advance directive does not automatically discontinue further care. It simply provides guidance to healthcare providers on the client's wishes for medical treatment. It is important for the nurse to explain this to the client and ensure that they understand the purpose of an advance directive.
B. Initiate a power of atorney for health care document.
While nurses can provide information and support the client in understanding the importance of having a power of attorney for healthcare, initiating such documents is typically not within the scope of nursing practice. This task usually requires legal guidance and formalities that go beyond nursing responsibilities.
C. Document that the provider discussed do-not-resuscitate status with the client.
Accurate documentation is crucial in healthcare. If a provider discusses do-not-resuscitate (DNR) status with a client, it must be documented in the client's medical record to ensure that all healthcare team members are aware of the client’s wishes.
D. Provide the client with written information about advance directives.
It is important for the nurse to provide the client with writen information about advance directives, including their rights and options for creating an advance directive. This information should be provided in a clear and understandable manner.
E. Communicate advance directives status via the medical record and shift report.
The nurse should communicate the client's advance directives status to other members of the healthcare team via the medical record and shift report. This ensures that everyone involved in the client's care is aware of the client's wishes and can provide care that is consistent with those wishes.
F. Instruct the client that an advance directive is a legal document and must be honored by care providers.
The nurse should instruct the client that an advance directive is a legal document that must be honored by care providers. This ensures that the client understands the importance of their advance directive and can advocate for their wishes if necessary.
Full Explanation
c, d, e, and f.
a. An advance directive does not automatically discontinue further care. It simply provides guidance to healthcare providers on the client's wishes for medical treatment. It is important for the nurse to explain this to the client and ensure that they understand the purpose of an advance directive.
b. While nurses can provide information and support the client in understanding the importance of having a power of attorney for healthcare, initiating such documents is typically not within the scope of nursing practice. This task usually requires legal guidance and formalities that go beyond nursing responsibilities.
c. Accurate documentation is crucial in healthcare. If a provider discusses do-not-resuscitate (DNR) status with a client, it must be documented in the client's medical record to ensure that all healthcare team members are aware of the client’s wishes.
d. Provide the client with writen information about advance directives: It is important for the nurse to provide the client with writen information about advance directives, including their rights and options for creating an advance directive. This information should be provided in a clear and understandable manner.
e. Communicate advance directives status via the medical record and shift report: The nurse should communicate the client's advance directives status to other members of the healthcare team via the medical record and shift report. This ensures that everyone involved in the client's care is aware of the client's wishes and can provide care that is consistent with those wishes.
f. Instruct the client that an advance directive is a legal document and must be honored by care providers: The nurse should instruct the client that an advance directive is a legal document that must be honored by care providers. This ensures that the client understands the importance of their advance directive and can advocate for their wishes if necessary.