Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
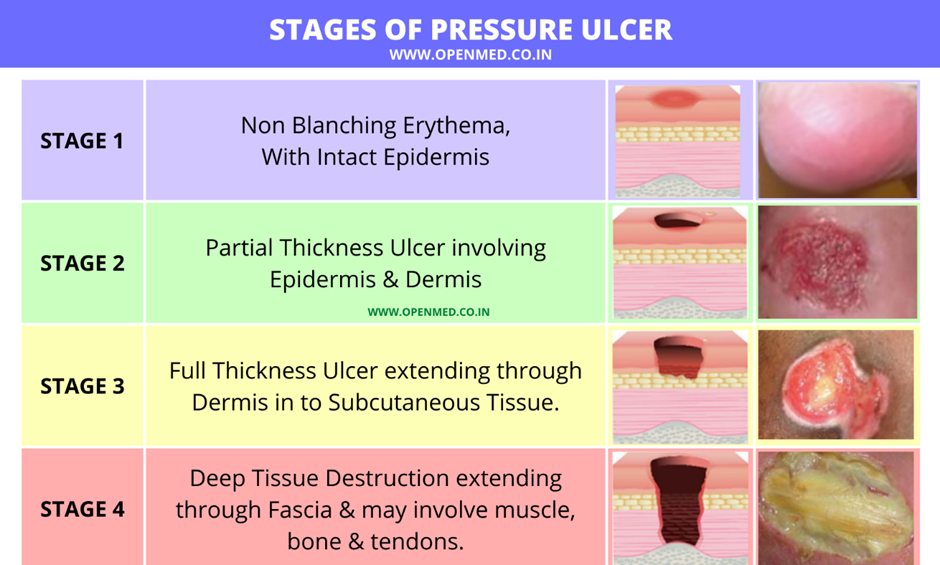
A nurse is collecting data on a client who has a stage 2 pressure injury. Which of the following findings should the nurse expect?
A. Intact skin with localized erythema.
Intact skin with localized erythema:Explanation: This description is more consistent with a stage 1 pressure injury, where there is non-blanchable erythema.
B. Full thickness skin loss with visible bone
Full thickness skin loss with visible bone:Explanation: This description is more consistent with a stage 4 pressure injury, which involves extensive tissue loss, including exposure of bone.
C. Full thickness skin loss with visible adipose tissue.
Full thickness skin loss with visible adipose tissue: Explanation: This finding is characteristic of a stage 3 pressure injury, where the loss of tissue extends down to the subcutaneous layer.
D. Partial-thickness skin loss with red tissue in wound bed.
Partial-thickness skin loss with red tissue in the wound bed:Explanation: This description is consistent with a stage 2 pressure injury, where there is partial-thickness skin loss involving the epidermis and possibly the dermis, forming a shallow open ulcer with a red-pink wound bed.
This question is an excerpt from Nurse Dive's nursing test bank - ATI LPN Proctored Exam. Take the full exam now
Full Explanation
A. Intact skin with localized erythema:
Explanation: This description is more consistent with a stage 1 pressure injury, where there is non-blanchable erythema.
B. Full thickness skin loss with visible bone:
Explanation: This description is more consistent with a stage 4 pressure injury, which involves extensive tissue loss, including exposure of bone.
C. Full thickness skin loss with visible adipose tissue:
Explanation: This finding is characteristic of a stage 3 pressure injury, where the loss of tissue extends down to the subcutaneous layer.
D. Partial-thickness skin loss with red tissue in the wound bed:
Explanation: This description is consistent with a stage 2 pressure injury, where there is partial-thickness skin loss involving the epidermis and possibly the dermis, forming a shallow open ulcer with a red-pink wound bed.
Similar Questions
A nurse is assisting with teaching a client who is on a low potassium diet. Which of the following instructions should the nurse include?
A. Choose orange juice instead of apple juice.
Choose orange juice instead of apple juice:Explanation: Orange juice is a source of potassium, so this choice would not be appropriate for a low potassium diet.
B. Replace sugar with molasses when baking.
Replace sugar with molasses when baking:Explanation: Molasses is a good alternative to sugar and does not contribute significantly to potassium intake, making it suitable for a low potassium diet.
C. Avoid using salt substitutes when cooking.
Avoid using salt substitutes when cooking: Explanation: Salt substitutes often contain potassium chloride, which can increase potassium intake. Therefore, it's advisable to avoid them on a low potassium diet.
D. Eat granola for breakfast.
Eat granola for breakfast:Explanation: Granola can be a good source of potassium, so it may not be suitable for someone on a low potassium diet.
Full Explanation
A. Choose orange juice instead of apple juice:
Explanation: Orange juice is a source of potassium, so this choice would not be appropriate for a low potassium diet.
B. Replace sugar with molasses when baking:
Explanation: Molasses is a good alternative to sugar and does not contribute significantly to potassium intake, making it suitable for a low potassium diet.
C. Avoid using salt substitutes when cooking:
Explanation: Salt substitutes often contain potassium chloride, which can increase potassium intake. Therefore, it's advisable to avoid them on a low potassium diet.
D. Eat granola for breakfast:
Explanation: Granola can be a good source of potassium, so it may not be suitable for someone on a low potassium diet.
A nurse is caring for a client who is receiving total parenteral nutrition (TPN) via an infusion pump. When collecting data about the client receiving this therapy, which of the following factors should the nurse monitor?
A. Height of the IV pole
Height of the IV pole:Explanation: The height of the IV pole is important for controlling the rate of the TPN infusion. Adjusting the height can regulate the flow rate.
B. IV insertion site
IV insertion site:Explanation: Monitoring the IV insertion site is crucial to assess for signs of infection, inflammation, or infiltration, which can compromise the effectiveness of TPN.
C. Manifestations of hypoglycemia
Manifestations of hypoglycemia: Explanation: TPN often contains glucose, and monitoring for signs of hypoglycemia is important, as abrupt cessation of TPN can lead to low blood glucose levels.
D. The client's oral intake
The client's oral intake:Explanation: Since the client is receiving TPN, their oral intake is not the primary source of nutrition. TPN provides essential nutrients intravenously.
Full Explanation
A. Height of the IV pole:
Explanation: The height of the IV pole is important for controlling the rate of the TPN infusion. Adjusting the height can regulate the flow rate.
B. IV insertion site:
Explanation: Monitoring the IV insertion site is crucial to assess for signs of infection, inflammation, or infiltration, which can compromise the effectiveness of TPN.
C. Manifestations of hypoglycemia:
Explanation: TPN often contains glucose, and monitoring for signs of hypoglycemia is important, as abrupt cessation of TPN can lead to low blood glucose levels.
D. The client's oral intake:
Explanation: Since the client is receiving TPN, their oral intake is not the primary source of nutrition. TPN provides essential nutrients intravenously.
A nurse is reviewing the laboratory results of a client who has a pressure ulcer. The nurse should identify an elevation in which of the following laboratory values as an indication that the client has developed an infection?
A. BUN
BUN (Blood Urea Nitrogen):Explanation: BUN is a measure of kidney function and hydration status. It is not typically elevated in response to a localized infection like a pressure ulcer.
B. WBC count
WBC count (White Blood Cell count):Explanation: An elevation in the WBC count is a common indicator of infection. Increased white blood cells suggest the body's immune response to an infection.
C. Potassium
Potassium: Explanation: Potassium levels are not typically used to indicate the presence of infection. Elevated potassium may be seen in conditions affecting kidney function.
D. RBC count
RBC count (Red Blood Cell count):Explanation: The RBC count is not a specific marker for infection. It is more related to issues such as anemia or oxygen-carrying capacity.
Full Explanation
A. BUN (Blood Urea Nitrogen):
Explanation: BUN is a measure of kidney function and hydration status. It is not typically elevated in response to a localized infection like a pressure ulcer.
B. WBC count (White Blood Cell count):
Explanation: An elevation in the WBC count is a common indicator of infection. Increased white blood cells suggest the body's immune response to an infection.
C. Potassium:
Explanation: Potassium levels are not typically used to indicate the presence of infection. Elevated potassium may be seen in conditions affecting kidney function.
D. RBC count (Red Blood Cell count):
Explanation: The RBC count is not a specific marker for infection. It is more related to issues such as anemia or oxygen-carrying capacity.