Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is completing an assessment following suctioning of a child who has a tracheostomy. Which of the following findings should the nurse identify as an indication that the procedure has been effective?
A. Increased respiratory rate
Increased respiratory rate: An increased respiratory rate may indicate that the child is experiencing respiratory distress or discomfort, which could be a sign that suctioning was not effective or that it was too aggressive. Ideally, after suctioning, the child's respiratory rate should stabilize or decrease as they are able to breathe more comfortably with a clear airway.
B. Decreased oxygen saturation
Decreased oxygen saturation: A decreased oxygen saturation level may indicate that the child is not receiving enough oxygen, which could be a sign of ineffective suctioning or airway obstruction. Effective suctioning should improve oxygenation by removing secretions and allowing for better airflow. A decrease in oxygen saturation would suggest the need for further assessment and intervention.
C. Clear breath sounds
Clear breath sounds: This is the correct option. Clear breath sounds indicate that the airway has been effectively cleared of excess secretions, allowing for clear airflow. After suctioning, the nurse should listen for clear breath sounds without any crackles, wheezes, or other abnormal sounds indicating obstruction or congestion.
D. Increased oral secretions
Increased oral secretions: Increased oral secretions may suggest that suctioning was not effective in clearing secretions from the airway, leading to pooling of secretions in the mouth. Effective suctioning should remove excess secretions from the airway, reducing the need for excessive oral secretions.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Nursing Care Of Children Proctored Exam. Take the full exam now
Full Explanation
A. Increased respiratory rate: An increased respiratory rate may indicate that the child is experiencing respiratory distress or discomfort, which could be a sign that suctioning was not effective or that it was too aggressive. Ideally, after suctioning, the child's respiratory rate should stabilize or decrease as they are able to breathe more comfortably with a clear airway.
B. Decreased oxygen saturation: A decreased oxygen saturation level may indicate that the child is not receiving enough oxygen, which could be a sign of ineffective suctioning or airway obstruction. Effective suctioning should improve oxygenation by removing secretions and allowing for better airflow. A decrease in oxygen saturation would suggest the need for further assessment and intervention.
C. Clear breath sounds: This is the correct option. Clear breath sounds indicate that the airway has been effectively cleared of excess secretions, allowing for clear airflow. After suctioning, the nurse should listen for clear breath sounds without any crackles, wheezes, or other abnormal sounds indicating obstruction or congestion.
D. Increased oral secretions: Increased oral secretions may suggest that suctioning was not effective in clearing secretions from the airway, leading to pooling of secretions in the mouth. Effective suctioning should remove excess secretions from the airway, reducing the need for excessive oral secretions.
Similar Questions
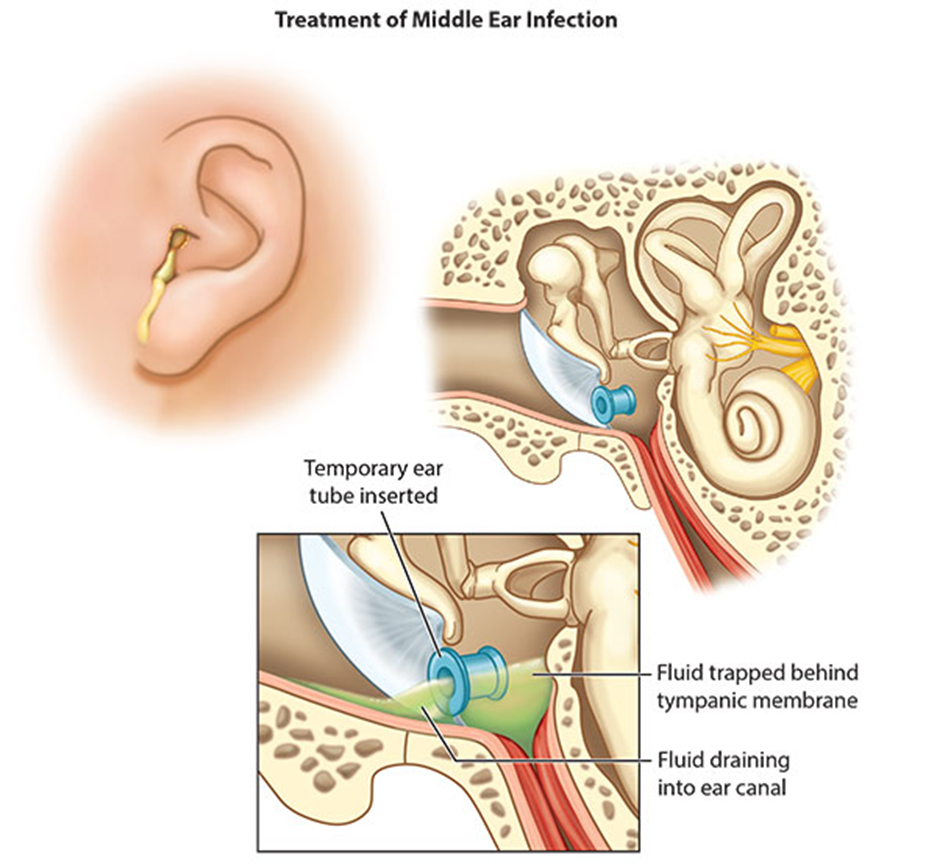
A nurse working on an outpatient surgical unit is providing discharge teaching to the parent of a preschooler following placement of tympanoplasty tubes. The parent asks the nurse, "What should I do if the tubes fall out?" Which of the following responses should the nurse make?
A. "Gently put the tubes back into the child's ears."
"Gently put the tubes back into the child's ears": This is not the correct response. Tympanoplasty tubes are not meant to be reinserted if they fall out. Attempting to reinsert them without proper medical training could cause injury or damage to the child's ears. Therefore, this response should be avoided.
B. "Bring the child to the emergency department immediately."
"Bring the child to the emergency department immediately": While it's important for the parent to seek medical attention if the tubes fall out, it may not always necessitate a visit to the emergency department, especially if the child is not experiencing any other symptoms. This response might cause unnecessary panic for the parent and may not be the most appropriate course of action.
C. "Notify the provider that the tubes have fallen out."
"Notify the provider that the tubes have fallen out": This is the correct response. If the tympanoplasty tubes fall out, the parent should notify the healthcare provider who performed the procedure. The provider can then assess the situation and determine the next steps, which may include scheduling a follow-up appointment to evaluate the child's ears.
D. "The tubes are sutured in place and must be surgically removed."
"The tubes are sutured in place and must be surgically removed": This is incorrect. Tympanoplasty tubes are not sutured in place; they are typically designed to fall out on their own after a certain period of time. Additionally, removal of tympanoplasty tubes usually does not require another surgical procedure.
Full Explanation
A. "Gently put the tubes back into the child's ears": This is not the correct response. Tympanoplasty tubes are not meant to be reinserted if they fall out. Attempting to reinsert them without proper medical training could cause injury or damage to the child's ears. Therefore, this response should be avoided.
B. "Bring the child to the emergency department immediately": While it's important for the parent to seek medical attention if the tubes fall out, it may not always necessitate a visit to the emergency department, especially if the child is not experiencing any other symptoms. This response might cause unnecessary panic for the parent and may not be the most appropriate course of action.
C. "Notify the provider that the tubes have fallen out": This is the correct response. If the tympanoplasty tubes fall out, the parent should notify the healthcare provider who performed the procedure. The provider can then assess the situation and determine the next steps, which may include scheduling a follow-up appointment to evaluate the child's ears.
D. "The tubes are sutured in place and must be surgically removed": This is incorrect. Tympanoplasty tubes are not sutured in place; they are typically designed to fall out on their own after a certain period of time. Additionally, removal of tympanoplasty tubes usually does not require another surgical procedure.
A home health nurse is providing teaching about postseizure management to the parents of a school-age child who has epilepsy and experiences tonic-clonic seizures. Which of the following instructions should the nurse include in the teaching? (Select all that apply.)
A. "Hyperextend your child's head for 5 minutes following a seizure."
"Hyperextend your child's head for 5 minutes following a seizure."This instruction is incorrect. Hyperextending the head after a seizure is not recommended and could potentially cause harm. Instead, it's important to ensure that the child's airway is clear and maintain a safe and comfortable position.
B. "Immediately following a seizure, give your child 6 ounces of water."
"Immediately following a seizure, give your child 6 ounces of water."This instruction is not necessary unless the child specifically requests water or appears to be dehydrated. It's important to focus on ensuring the child's safety and comfort immediately after a seizure.
C. "Following a seizure, record the length and characteristics of your child's seizure."
"Following a seizure, record the length and characteristics of your child's seizure."This instruction is correct. Keeping a record of the length and characteristics of the child's seizures can provide valuable information to healthcare providers for managing the child's epilepsy and adjusting treatment as needed.
D. "Administer rectal diazepam to your child following a seizure."
"Administer rectal diazepam to your child following a seizure."This instruction may be appropriate in some cases, particularly if the child's seizures are prolonged or if they have a history of status epilepticus. However, the administration of rectal diazepam should be done according to the healthcare provider's instructions and with proper training.
E. "Call for emergency medical services if the size of your child's pupils are unequal after a seizure."
This instruction is correct. Unequal pupil size (anisocoria) after a seizure could indicate a serious underlying condition and should prompt immediate medical evaluation. It's important for the parents to be aware of this potential sign of concern and to seek prompt medical attention if it occurs.
Full Explanation
A. "Hyperextend your child's head for 5 minutes following a seizure."
This instruction is incorrect. Hyperextending the head after a seizure is not recommended and could potentially cause harm. Instead, it's important to ensure that the child's airway is clear and maintain a safe and comfortable position.
B. "Immediately following a seizure, give your child 6 ounces of water."
This instruction is not necessary unless the child specifically requests water or appears to be dehydrated. It's important to focus on ensuring the child's safety and comfort immediately after a seizure.
C. "Following a seizure, record the length and characteristics of your child's seizure."
This instruction is correct. Keeping a record of the length and characteristics of the child's seizures can provide valuable information to healthcare providers for managing the child's epilepsy and adjusting treatment as needed.
D. "Administer rectal diazepam to your child following a seizure."
This instruction may be appropriate in some cases, particularly if the child's seizures are prolonged or if they have a history of status epilepticus. However, the administration of rectal diazepam should be done according to the healthcare provider's instructions and with proper training.
E. "Call for emergency medical services if the size of your child's pupils are unequal after a seizure."
This instruction is correct. Unequal pupil size (anisocoria) after a seizure could indicate a serious underlying condition and should prompt immediate medical evaluation. It's important for the parents to be aware of this potential sign of concern and to seek prompt medical attention if it occurs.
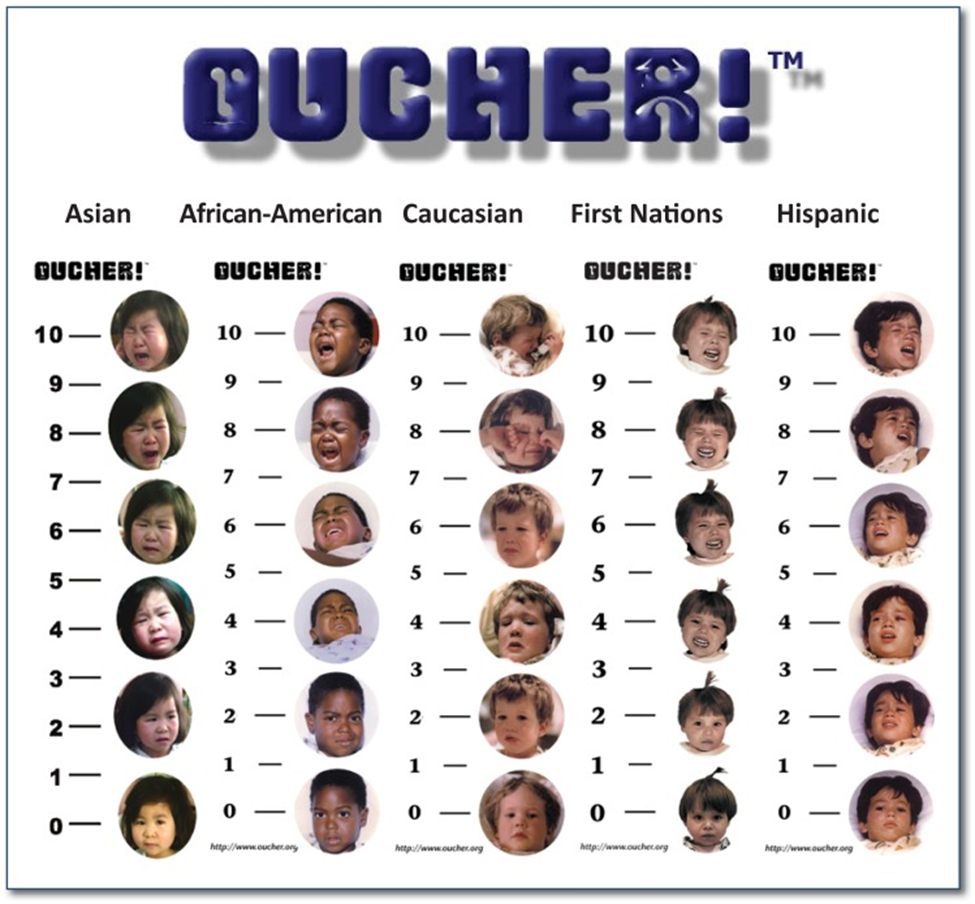
A nurse is assessing a 4-year-old child following a surgical procedure. Which of the following pain rating scales should the nurse use?
A. Oucher pain rating scale
Oucher pain rating scale: The Oucher pain rating scale uses pictures of children's faces to represent varying degrees of pain intensity. This scale is specifically designed for young children and can be effective in assessing pain in preschool-aged children who may not yet be able to accurately use verbal descriptors to express their pain.
B. Word-Graphic rating scale
Word-Graphic rating scale: This type of scale presents both words and pictures to represent different levels of pain intensity. While it may be suitable for older children who can understand and use words to describe their pain, it may be less effective for a 4-year-old child who is still developing language skills.
C. Numeric rating scale
Numeric rating scale: Numeric rating scales typically ask the child to rate their pain on a scale from 0 to 10, with 0 representing no pain and 10 representing the worst pain imaginable. While this scale may be appropriate for older children, it may be challenging for a 4-year-old to understand and use numbers to describe their pain.
D. Visual analog scale
Visual analog scale: Visual analog scales typically consist of a line with endpoints labeled "no pain" and "worst pain imaginable," with the child asked to mark or point to the spot on the line that represents their pain level. While this scale may be suitable for older children and adults, it may be too abstract for a 4-year-old child to understand and use effectively.
Full Explanation
A. Oucher pain rating scale: The Oucher pain rating scale uses pictures of children's faces to represent varying degrees of pain intensity. This scale is specifically designed for young children and can be effective in assessing pain in preschool-aged children who may not yet be able to accurately use verbal descriptors to express their pain.
B. Word-Graphic rating scale: This type of scale presents both words and pictures to represent different levels of pain intensity. While it may be suitable for older children who can understand and use words to describe their pain, it may be less effective for a 4-year-old child who is still developing language skills.
C. Numeric rating scale: Numeric rating scales typically ask the child to rate their pain on a scale from 0 to 10, with 0 representing no pain and 10 representing the worst pain imaginable. While this scale may be appropriate for older children, it may be challenging for a 4-year-old to understand and use numbers to describe their pain.
D. Visual analog scale: Visual analog scales typically consist of a line with endpoints labeled "no pain" and "worst pain imaginable," with the child asked to mark or point to the spot on the line that represents their pain level. While this scale may be suitable for older children and adults, it may be too abstract for a 4-year-old child to understand and use effectively.