Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is monitoring an infant who is receiving opioids for pain.
Which of the following findings should indicate to the nurse that the medication is having a therapeutic effect?
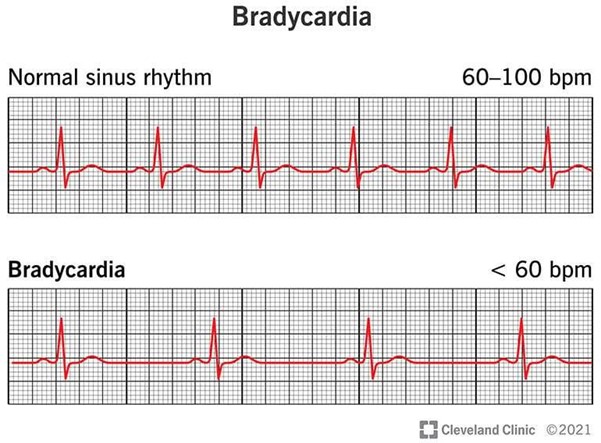
A. Bradycardia.
Choice A is wrong because bradycardia is not an indication that the medication is having a therapeutic effect.
B. Relaxed facial expression.
A relaxed facial expression can indicate that the medication is having a therapeutic effect and that the infant is experiencing pain relief.
C. Increased blood pressure.
Choice C is wrong because increased blood pressure is not an indication that the medication is having a therapeutic effect.
D. Limb withdrawal.
Choice D is wrong because limb withdrawal is not an indication that the medication is having a therapeutic effect.
This question is an excerpt from Nurse Dive's nursing test bank - ATI RN Nursing Care of Children 2019 Proctored Exam. Take the full exam now
Full Explanation
A relaxed facial expression can indicate that the medication is having a therapeutic effect and that the infant is experiencing pain relief.
Choice A is wrong because bradycardia is not an indication that the medication is having a therapeutic effect.
Choice C is wrong because increased blood pressure is not an indication that the medication is having a therapeutic effect.
Choice D is wrong because limb withdrawal is not an indication that the medication is having a therapeutic effect.
Similar Questions
A nurse is assessing a 5-month-old infant.
Which of the following findings should the nurse report to the provider?
A. Unable to hold a bottle.
Unable to hold a bottle At around 6 months of age, some babies can hold their own bottle. This is not a concerning finding for a 5-month-old infant. Therefore, this is not the correct answer.
B. Unable to roll from back to abdomen.
Unable to roll from back to abdomen Rolling over often starts around 4-6 months, so it’s not unusual for a 5-month-old to still be developing this skill. Therefore, this is not the correct answer.
C. Absent grasp reflex.
Absent grasp reflex The grasp reflex is an involuntary movement that your baby starts making in utero and continues doing until around 6 months of age. The grasp reflex lasts until the baby is about 5 to 6 months old. Therefore, this is not the correct answer.
D. Exhibits head lag when pulled to a sitting position.
Exhibits head lag when pulled to a sitting position By the age of 5 months, most infants have developed enough strength in their neck and upper body to control their head movement. This means they should not exhibit a significant head lag when pulled to a sitting position1. If this is not the case, it could indicate a delay in motor development or a potential neurological issue, which should be reported to the healthcare provider for further evaluation. Therefore, this is the correct answer.
Full Explanation
The correct answer is d. Exhibits head lag when pulled to a sitting position.
Choice A: Unable to hold a bottle At around 6 months of age, some babies can hold their own bottle. This is not a concerning finding for a 5-month-old infant. Therefore, this is not the correct answer.
Choice B: Unable to roll from back to abdomen Rolling over often starts around 4-6 months, so it’s not unusual for a 5-month-old to still be developing this skill. Therefore, this is not the correct answer.
Choice C: Absent grasp reflex The grasp reflex is an involuntary movement that your baby starts making in utero and continues doing until around 6 months of age. The grasp reflex lasts until the baby is about 5 to 6 months old. Therefore, this is not the correct answer.
Choice D: Exhibits head lag when pulled to a sitting position By the age of 5 months, most infants have developed enough strength in their neck and upper body to control their head movement. This means they should not exhibit a significant head lag when pulled to a sitting position1. If this is not the case, it could indicate a delay in motor development or a potential neurological issue, which should be reported to the healthcare provider for further evaluation. Therefore, this is the correct answer.
A nurse in a pediatric clinic is providing teaching to the guardian of an infant who has a new prescription for digoxin.
Which of the following manifestations should the nurse include as an indication of digoxin toxicity?
A. Polyuria.
Choice A is wrong because polyuria is not a sign of digoxin toxicity.
B. Diaphoresis.
Choice B is wrong because diaphoresis is not a sign of digoxin toxicity.
C. Bradycardia.
Bradycardia, or a slow heart rate, is a sign of digoxin toxicity in infants. Digoxin is a medication used to improve the strength and efficiency of the heart and to control the rate and rhythm of the heartbeat. However, an overdose can cause changes in the rate or rhythm of the heartbeat, including bradycardia.
D. Jaundice.
Choice D is wrong because jaundice is not a sign of digoxin toxicity.
Full Explanation
Bradycardia, or a slow heart rate, is a sign of digoxin toxicity in infants.
Digoxin is a medication used to improve the strength and efficiency of the heart and to control the rate and rhythm of the heartbeat.
However, an overdose can cause changes in the rate or rhythm of the heartbeat, including bradycardia.
Choice A is wrong because polyuria is not a sign of digoxin toxicity.
Choice B is wrong because diaphoresis is not a sign of digoxin toxicity.
Choice D is wrong because jaundice is not a sign of digoxin toxicity.
A nurse is assessing an infant who has severe dehydration due to gastroenteritis.
Which of the following findings should the nurse expect?
A. Hypertension.
Choice A is wrong because hypertension is not a sign of severe dehydration in infants.
B. Increased urine output.
Choice B is wrong because increased urine output is not a sign of severe dehydration in infants. In fact, decreased urine output is a sign of dehydration 2.
C. Capillary refill of 2 seconds.
Choice C is wrong because a capillary refill of 2 seconds is normal and not a sign of severe dehydration in infants.
D. Increased respiratory rate.
An increased respiratory rate is a sign of severe dehydration in infants. Dehydration occurs when an infant loses so much body fluid that they are not able to maintain ordinary function.
E. Increased respiratory rate.
Full Explanation
An increased respiratory rate is a sign of severe dehydration in infants.
Dehydration occurs when an infant loses so much body fluid that they are not able to maintain ordinary function.
Choice A is wrong because hypertension is not a sign of severe dehydration in infants.
Choice B is wrong because increased urine output is not a sign of severe dehydration in infants.
In fact, decreased urine output is a sign of dehydration 2.
Choice C is wrong because a capillary refill of 2 seconds is normal and not a sign of severe dehydration in infants.