Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is performing a focused assessment for a client's vision. What visual assessment is the nurse making when she extends her hand for the client to shake?
A. Depth perception
Reason: Depth perception is the ability to judge the distance and position of objects in three-dimensional space. Depth perception is assessed by asking the client to touch the tip of a pen or pencil held by the nurse, or by using a stereopsis test.
B. Peripheral vision
Reason: Peripheral vision is the ability to see objects and movements outside the direct line of vision. Peripheral vision is assessed by asking the client to shake the hand of the nurse, who stands at an angle to the client's side, or by using a confrontation test.
C. Color deficit
Reason: Color deficit is the inability to distinguish certain colors or shades of colors. Color deficit is assessed by asking the client to identify numbers or shapes on a color plate test, such as the Ishihara test.
D. Double vision
Reason: Double vision is the perception of two images of a single object. Double vision is assessed by asking the client to cover one eye and look at an object, then switch eyes and compare the images, or by using a cover-uncover test.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: Depth perception is the ability to judge the distance and position of objects in three-dimensional space. Depth perception is assessed by asking the client to touch the tip of a pen or pencil held by the nurse, or by using a stereopsis test.
Choice B Reason: Peripheral vision is the ability to see objects and movements outside the direct line of vision. Peripheral vision is assessed by asking the client to shake the hand of the nurse, who stands at an angle to the client's side, or by using a confrontation test.
Choice C Reason: Color deficit is the inability to distinguish certain colors or shades of colors. Color deficit is assessed by asking the client to identify numbers or shapes on a color plate test, such as the Ishihara test.
Choice D Reason: Double vision is the perception of two images of a single object. Double vision is assessed by asking the client to cover one eye and look at an object, then switch eyes and compare the images, or by using a cover-uncover test.
Similar Questions
A nurse collects the health history of a 65-year-old client. Which of the following risk factors in the client's history puts the client at the highest risk for embolic stroke?
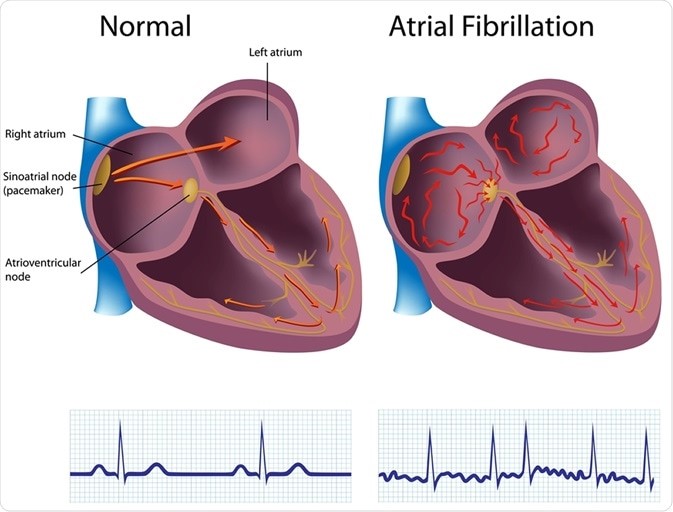
A. Atrial fibrillation.
reason: This is the correct answer because atrial fibrillation is the risk factor that puts the client at the highest risk for embolic stroke. Atrial fibrillation is an irregular and rapid heart rate that causes poor blood flow and blood pooling in the heart chambers. This can lead to the formation of blood clots that can travel to the brain and block an artery, causing an embolic stroke.
B. Hypertension.
reason: This is incorrect because hypertension is not the risk factor that puts the client at the highest risk for embolic stroke. Hypertension is high blood pressure that puts stress on the blood vessels and increases the risk of bleeding or rupture. This can lead to a hemorrhagic stroke, but not an embolic stroke.
C. Diabetes.
reason: This is incorrect because diabetes is not the risk factor that puts the client at the highest risk for embolic stroke. Diabetes is a condition that causes high blood sugar levels and damages the blood vessels and nerves. This can lead to poor circulation and increased risk of infection and ulcers, but not an embolic stroke.
D. Alcohol abuse.
reason: This is incorrect because alcohol abuse is not the risk factor that puts the client at the highest risk for embolic stroke. Alcohol abuse is excessive consumption of alcohol that affects liver function and blood clotting factors. This can lead to liver disease and bleeding disorders, but not an embolic stroke.
Full Explanation
Choice A reason: This is the correct answer because atrial fibrillation is the risk factor that puts the client at
the highest risk for embolic stroke. Atrial fibrillation is an irregular and rapid heart rate that causes poor blood flow and blood pooling in the heart chambers. This can lead to the formation of blood clots that can travel to the brain and block an artery, causing an embolic stroke.
Choice B reason: This is incorrect because hypertension is not the risk factor that puts the client at
the highest risk for embolic stroke. Hypertension is high blood pressure that puts stress on the blood vessels and increases the risk of bleeding or rupture. This can lead to a hemorrhagic stroke, but not an embolic stroke.
Choice C reason: This is incorrect because diabetes is not the risk factor that puts the client at
the highest risk for embolic stroke. Diabetes is a condition that causes high blood sugar levels and damages the blood vessels and nerves. This can lead to poor circulation and increased risk of infection and ulcers, but not an embolic stroke.
Choice D reason: This is incorrect because alcohol abuse is not the risk factor that puts the client at
the highest risk for embolic stroke. Alcohol abuse is excessive consumption of alcohol that affects liver function and blood clotting factors. This can lead to liver disease and bleeding disorders, but not an embolic stroke.
A nurse is reviewing the medical record of a client who is experiencing delirium. Which of the following in the health record should the nurse identify as a cause of this disorder?
A. Seasonal allergies
Reason: Seasonal allergies are not a cause of delirium, but a common condition that affects the respiratory system and causes symptoms such as sneezing, runny nose, itchy eyes, or coughing.
B. History of GERD
Reason: History of GERD is not a cause of delirium, but a chronic condition that affects the digestive system and causes symptoms such as heartburn, regurgitation, chest pain, or difficulty swallowing.
C. Benzodiazepines
Reason: Benzodiazepines are a cause of delirium, especially in older adults or those with cognitive impairment. Benzodiazepines are a class of drugs that act on the central nervous system and cause sedation, relaxation, and reduced anxiety. However, they can also impair memory, attention, orientation, and judgment, and lead to confusion, agitation, hallucinations, or delusions.
D. Completed antibiotics 10 days ago
Reason: Completed antibiotics 10 days ago are not a cause of delirium, but a treatment for bacterial infections. Antibiotics can have side effects such as nausea, diarrhea, rash, or allergic reactions, but they do not cause delirium unless they are toxic or interact with other medications.
Full Explanation
Choice A Reason: Seasonal allergies are not a cause of delirium, but a common condition that affects the respiratory system and causes symptoms such as sneezing, runny nose, itchy eyes, or coughing.
Choice B Reason: History of GERD is not a cause of delirium, but a chronic condition that affects the digestive system and causes symptoms such as heartburn, regurgitation, chest pain, or difficulty swallowing.
Choice C Reason: Benzodiazepines are a cause of delirium, especially in older adults or those with cognitive impairment. Benzodiazepines are a class of drugs that act on the central nervous system and cause sedation, relaxation, and reduced anxiety. However, they can also impair memory, attention, orientation, and judgment, and lead to confusion, agitation, hallucinations, or delusions.
Choice D Reason: Completed antibiotics 10 days ago are not a cause of delirium, but a treatment for bacterial infections. Antibiotics can have side effects such as nausea, diarrhea, rash, or allergic reactions, but they do not cause delirium unless they are toxic or interact with other medications.
A nurse is assessing a client who has a score of 6 on the Glasgow Coma Scale. The nurse should expect which of the following outcomes based on this score?
A. The client needs total nursing care.
Reason: The client needs total nursing care is the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which is a tool that measures the level of consciousness based on eye opening, verbal response, and motor response. A score of 6 indicates severe brain injury and coma, meaning that the client is unresponsive and dependent on others for all activities of daily living.
B. Indicates stable neurologic status
Reason: Indicates stable neurologic status is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. A stable neurologic status means that there are no changes in the level of consciousness, vital signs, or neurological signs.
C. The client has a decline in level of consciousness but is able to protect his airway
Reason: The client has a decline in level of consciousness but is able to protect his airway is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. A decline in level of consciousness means that the client is less alert and responsive than normal, but still able to respond to stimuli and maintain airway patency.
D. The client is alert and oriented.
Reason: The client is alert and oriented is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. Alert and oriented means that the client is fully awake and aware of person, place, time, and situation.
Full Explanation
Choice A Reason: The client needs total nursing care is the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which is a tool that measures the level of consciousness based on eye opening, verbal response, and motor response. A score of 6 indicates severe brain injury and coma, meaning that the client is unresponsive and dependent on others for all activities of daily living.
Choice B Reason: Indicates stable neurologic status is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. A stable neurologic status means that there are no changes in the level of consciousness, vital signs, or neurological signs.
Choice C Reason: The client has a decline in level of consciousness but is able to protect his airway is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. A decline in level of consciousness means that the client is less alert and responsive than normal, but still able to respond to stimuli and maintain airway patency.
Choice D Reason: The client is alert and oriented is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. Alert and oriented means that the client is fully awake and aware of person, place, time, and situation.