Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is performing a focused assessment for vision on a client suspected of having vision loss. Which cranial nerve is the nurse assessing when determining if there are visual field or visual acuity deficits?
A. Cranial Nerve VIII
Reason: This choice is incorrect. Cranial Nerve VIII is the vestibulocochlear nerve, which is responsible for hearing and balance. It does not affect vision or eye movements.
B. Cranial Nerve II
Reason: This is the correct choice. Cranial Nerve II is the optic nerve, which is responsible for transmitting visual information from the retina to the brain. It affects visual field and visual acuity, which are measures of peripheral and central vision, respectively.
C. Cranial Nerve I
Reason: This choice is incorrect. Cranial Nerve I is the olfactory nerve, which is responsible for smell. It does not affect vision or eye movements.
D. Cranial Nerve VII
Reason: This choice is incorrect. Cranial Nerve VII is the facial nerve, which is responsible for facial expressions and taste. It does not affect vision or eye movements.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: This choice is incorrect. Cranial Nerve VIII is the vestibulocochlear nerve, which is responsible for hearing and balance. It does not affect vision or eye movements.
Choice B Reason: This is the correct choice. Cranial Nerve II is the optic nerve, which is responsible for transmitting visual information from the retina to the brain. It affects visual field and visual acuity, which are measures of peripheral and central vision, respectively.
Choice C Reason: This choice is incorrect. Cranial Nerve I is the olfactory nerve, which is responsible for smell. It does not affect vision or eye movements.
Choice D Reason: This choice is incorrect. Cranial Nerve VII is the facial nerve, which is responsible for facial expressions and taste. It does not affect vision or eye movements.
Similar Questions
When performing an assessment, the nurse observes for bilateral equality. After performing a neurological assessment, which of the following will the nurse document when assessment findings indicate that there is left facial droop?
A. Inability to perform within normal limits
Reason: This choice is incorrect. Inability to perform within normal limits is a vague and general term that does not describe the specific finding of left facial droop. The nurse should document the exact observation and compare it to the expected or normal range.
B. Symmetrical findings
Reason: This choice is incorrect. Symmetrical findings mean that both sides of the body or face are equal or similar in appearance or function. Left facial droop indicates that one side of the face is lower or weaker than the other, which is not symmetrical.
C. Asymmetrical findings
Reason: This is the correct choice. Asymmetrical findings mean that both sides of the body or face are unequal or different in appearance or function. Left facial droop indicates that one side of the face is lower or weaker than the other, which is asymmetrical.
D. Bilateral strength present
Reason: This choice is incorrect. Bilateral strength present means that both sides of the body or face have normal or adequate muscle power or force. Left facial droop indicates that one side of the face has reduced or impaired muscle power or force, which is not bilateral strength present.
Full Explanation
Choice A Reason: This choice is incorrect. Inability to perform within normal limits is a vague and general term that does not describe the specific finding of left facial droop. The nurse should document the exact observation and compare it to the expected or normal range.
Choice B Reason: This choice is incorrect. Symmetrical findings mean that both sides of the body or face are equal or similar in appearance or function. Left facial droop indicates that one side of the face is lower or weaker than the other, which is not symmetrical.
Choice C Reason: This is the correct choice. Asymmetrical findings mean that both sides of the body or face are unequal or different in appearance or function. Left facial droop indicates that one side of the face is lower or weaker than the other, which is asymmetrical.
Choice D Reason: This choice is incorrect. Bilateral strength present means that both sides of the body or face have normal or adequate muscle power or force. Left facial droop indicates that one side of the face has reduced or impaired muscle power or force, which is not bilateral strength present.
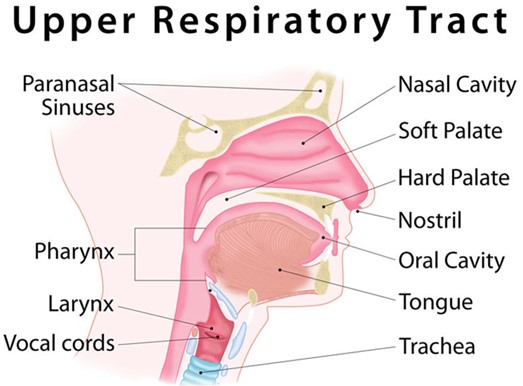
A client arrives with an upper respiratory infection and complains of otalgia, malaise, and nasal drainage. The client's temperature is 100.7 F. Which of the following will the nurse anticipate providing to the client?
A. Education about mastoidectomy
reason: This is incorrect because education about mastoidectomy is not relevant for a client with an upper respiratory infection. Mastoidectomy is a surgical procedure that removes part or all of the mastoid bone behind the ear, which can become infected or inflamed due to chronic or recurrent middle ear infections. The nurse should assess the client's ear for signs of mastoiditis, such as swelling, tenderness, or redness behind the ear, but mastoidectomy is not a common or first-line treatment for upper respiratory infection.
B. A referral for a hearing test
reason: This is incorrect because a referral for a hearing test is not necessary for a client with an upper respiratory infection. Hearing test is a diagnostic tool that measures how well a person can hear different sounds at different frequencies and intensities. The nurse should ask the client about any changes in hearing or tinnitus, which are possible complications of upper respiratory infection, but a hearing test is not a routine or urgent intervention for this condition.
C. Education on administration of oral antibiotics
reason: This is correct because education on the administration of oral antibiotics can help treat an upper respiratory infection. Antibiotics are drugs that kill or inhibit bacteria that cause infections. Upper respiratory infections can be caused by various pathogens, such as viruses, bacteria, or fungi, but bacterial infections are more likely to cause fever, otalgia, or purulent nasal drainage. The nurse should instruct the client on how to take antibiotics as prescribed, such as dosage, frequency, duration, side effects, and interactions.
D. A prescription for an antifungal cream
reason: This is incorrect because a prescription for an antifungal cream is not appropriate for a client with an upper respiratory infection. Antifungal cream is a topical medication that kills or inhibits fungi that cause skin infections. Upper respiratory infection is not a skin infection, but an infection of the nose, throat, or sinuses. Antifungal cream has no effect on upper respiratory infection and may cause adverse effects or resistance.
Full Explanation
Choice A reason: This is incorrect because education about mastoidectomy is not relevant for a client with an upper respiratory infection. Mastoidectomy is a surgical procedure that removes part or all of the mastoid bone behind the ear, which can become infected or inflamed due to chronic or recurrent middle ear infections. The nurse should assess
the client's ear for signs of mastoiditis, such as swelling, tenderness, or redness behind the ear, but mastoidectomy is not a common or first-line treatment for upper respiratory infection.
Choice B reason: This is incorrect because a referral for a hearing test is not necessary for a client with an upper respiratory infection. Hearing test is a diagnostic tool that measures how well a person can hear different sounds at different frequencies and intensities. The nurse should ask the client about any changes in hearing or tinnitus, which are possible complications of upper respiratory infection, but a hearing test is not a routine or urgent intervention for this condition.
Choice C reason: This is correct because education on the administration of oral antibiotics can help treat an upper respiratory infection. Antibiotics are drugs that kill or inhibit bacteria that cause infections. Upper respiratory infections can be caused by various pathogens, such as viruses, bacteria, or fungi, but bacterial infections are more likely to cause fever, otalgia, or purulent nasal drainage. The nurse should instruct the client on how to take antibiotics as prescribed, such as dosage, frequency, duration, side effects, and interactions.
Choice D reason: This is incorrect because a prescription for an antifungal cream is not appropriate for a client with an upper respiratory infection. Antifungal cream is a topical medication that kills or inhibits fungi that cause skin infections. Upper respiratory infection is not a skin infection, but an infection of the nose, throat, or sinuses. Antifungal cream has no effect on upper respiratory infection and may cause adverse effects or resistance.
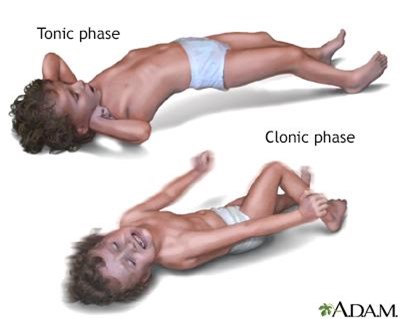
A nurse is caring for a client who is experiencing a seizure. Which of the following actions should the nurse take? (Select all that apply)
A. Place the client into a supine position.
Choice A Reason: This choice is incorrect. Placing the client into a supine position is not an action that the nurse should take, as it can compromise the airway and increase the risk of aspiration. The nurse should position the client on their side with their head tilted slightly forward to allow saliva and secretions to drain out of their mouth.
B. Apply restraints.
Choice B Reason: This choice is incorrect. Applying restraints is not an action that the nurse should take, as it can cause injury and increase agitation. The nurse should protect the client from harm by removing any objects or furniture that may cause harm and padding any hard surfaces with blankets or pillows.
C. Insert a bite stick into the client's mouth.
Choice C Reason: This choice is incorrect. Inserting a bite stick into the client's mouth is not an action that the nurse should take, as it can cause injury and obstruction. The nurse should never force anything into the client's mouth during a seizure, as it can damage their teeth, gums, tongue, or jaw.
D. Loosen restrictive clothing.
Choice D Reason: This is a correct choice. Loosening restrictive clothing is an action that the nurse should take, as it can improve breathing and circulation. The nurse should unbutton any tight collars, belts, or ties that may constrict the chest or neck.
E. Place a pillow under the client's head.
Choice E Reason: This is a correct choice. Placing a pillow under the client's head is an action that the nurse should take, as it can prevent injury and provide comfort. The nurse should support the client's head with a soft pillow or cushion to prevent hitting it against any hard surfaces.
Full Explanation
Choice A Reason: This choice is incorrect. Placing the client into a supine position is not an action that the nurse should take, as it can compromise the airway and increase the risk of aspiration. The nurse should position the client on their side with their head tilted slightly forward to allow saliva and secretions to drain out of their mouth.
Choice B Reason: This choice is incorrect. Applying restraints is not an action that the nurse should take, as it can cause injury and increase agitation. The nurse should protect the client from harm by removing any objects or furniture that may cause harm and padding any hard surfaces with blankets or pillows.
Choice C Reason: This choice is incorrect. Inserting a bite stick into the client's mouth is not an action that the nurse should take, as it can cause injury and obstruction. The nurse should never force anything into the client's mouth during a seizure, as it can damage their teeth, gums, tongue, or jaw.
Choice D Reason: This is a correct choice. Loosening restrictive clothing is an action that the nurse should take, as it can improve breathing and circulation. The nurse should unbutton any tight collars, belts, or ties that may constrict the chest or neck.
Choice E Reason: This is a correct choice. Placing a pillow under the client's head is an action that the nurse should take, as it can prevent injury and provide comfort. The nurse should support the client's head with a soft pillow or cushion to prevent hitting it against any hard surfaces.