Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is performing a Weber test on a client who reports difficulty hearing in his left ear. The client informs the nurse that he can hear the tone louder in his left ear. Which of the following does this result indicate?
A. The test is inconclusive
Reason: The test is not inconclusive, but rather positive for conductive hearing loss. The Weber test involves placing a vibrating tuning fork on the center of the forehead and asking the client which ear hears the sound louder. It can help differentiate between conductive and sensorineural hearing loss.
B. The client has conductive hearing loss
Reason: This is the correct choice. The client has conductive hearing loss, which is a type of hearing loss that occurs when sound waves are blocked or reduced in the outer or middle ear. It can be caused by earwax, infection, fluid, perforation, or trauma. In conductive hearing loss, the Weber test shows lateralization to the affected ear, meaning the sound is heard louder in that ear.
C. The client has normal hearing
Reason: The client does not have normal hearing, but rather conductive hearing loss. In normal hearing, the Weber test shows no lateralization, meaning the sound is heard equally in both ears.
D. The client has sensorineural hearing loss
Reason: The client does not have sensorineural hearing loss, but rather conductive hearing loss. Sensorineural hearing loss is a type of hearing loss that occurs when there is damage to the inner ear or auditory nerve. It can be caused by aging, noise exposure, disease, or drugs. In sensorineural hearing loss, the Weber test shows lateralization to the unaffected ear, meaning the sound is heard louder in that ear.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 4. Take the full exam now
Full Explanation
Choice A Reason: The test is not inconclusive, but rather positive for conductive hearing loss. The Weber test involves placing a vibrating tuning fork on the center of the forehead and asking the client which ear hears the sound louder. It can help differentiate between conductive and sensorineural hearing loss.
Choice B Reason: This is the correct choice. The client has conductive hearing loss, which is a type of hearing loss that occurs when sound waves are blocked or reduced in the outer or middle ear. It can be caused by earwax, infection, fluid, perforation, or trauma. In conductive hearing loss, the Weber test shows lateralization to the affected ear, meaning the sound is heard louder in that ear.
Choice C Reason: The client does not have normal hearing, but rather conductive hearing loss. In normal hearing, the Weber test shows no lateralization, meaning the sound is heard equally in both ears.
Choice D Reason: The client does not have sensorineural hearing loss, but rather conductive hearing loss. Sensorineural hearing loss is a type of hearing loss that occurs when there is damage to the inner ear or auditory nerve. It can be caused by aging, noise exposure, disease, or drugs. In sensorineural hearing loss, the Weber test shows lateralization to the unaffected ear, meaning the sound is heard louder in that ear.
Similar Questions
When providing information to a client in the rehabilitative phase of a burn injury, which of the following will the nurse identify as the goal?
A. Resume a functional role in society
reason: This is correct because resuming a functional role in society is the ultimate goal for a client in the rehabilitative phase of a burn injury. The rehabilitative phase begins when wound healing is complete and lasts until physical and psychosocial recovery is achieved. The nurse should help the client regain independence, self-esteem, and quality of life by providing education, counseling, referrals, and resources.
B. Pain management
reason: This is incorrect because pain management is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Pain management is important throughout all phases of burn care, but especially during wound healing and scar formation, which can cause itching, tightness, or hypersensitivity. The nurse should assess the client's pain level and administer analgesics, antipruritics, or moisturizers as ordered.
C. Provide continued full support to the client
reason: This is incorrect because providing continued full support to the client is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Providing continued full support to the client can help them cope with physical and emotional challenges, such as scarring, disfigurement, disability, or depression. The nurse should provide emotional support, active listening, positive feedback, and encouragement to the client.
D. Prevent infection
reason: This is incorrect because preventing infection is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Preventing infection is crucial during wound healing and grafting, which can be compromised by bacterial colonization or contamination. The nurse should monitor the client's vital signs, wound appearance, and laboratory results, and administer antibiotics or antiseptics as ordered.
Full Explanation
Choice A reason: This is correct because resuming a functional role in society is the ultimate goal for a client in the rehabilitative phase of a burn injury. The rehabilitative phase begins when wound healing is complete and lasts until physical and psychosocial recovery is achieved. The nurse should help the client regain independence, self-esteem, and quality of life by providing education, counseling, referrals, and resources.
Choice B reason: This is incorrect because pain management is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Pain management is important throughout all phases of burn care, but especially during wound healing and scar formation, which can cause itching, tightness, or hypersensitivity. The nurse should assess the client's pain level and administer analgesics, antipruritics, or moisturizers as ordered.
Choice C reason: This is incorrect because providing continued full support to the client is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Providing continued full support to the client can help them cope with physical and emotional challenges, such as scarring, disfigurement, disability, or depression. The nurse should provide emotional support, active listening, positive feedback, and encouragement to the client.
Choice D reason: This is incorrect because preventing infection is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Preventing infection is crucial during wound healing and grafting, which can be compromised by bacterial colonization or contamination. The nurse should monitor the client's vital signs, wound appearance, and laboratory results, and administer antibiotics or antiseptics as ordered.
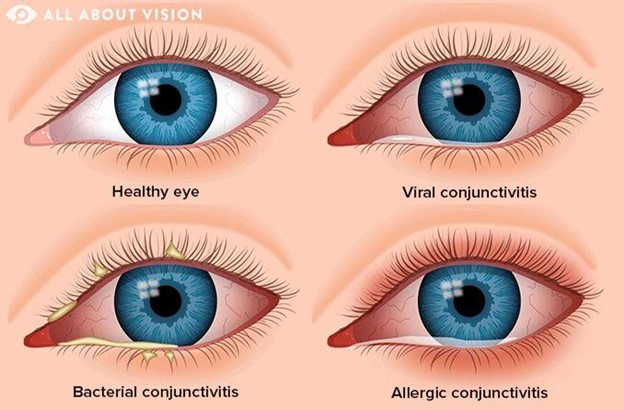
A client arrives with a pink eye that is itchy, swollen, and uncomfortable with a creamy discharge. Which of the following home care instructions will the nurse offer to the client?
A. Wash towels, sheets, and pillowcases
Reason: This is the correct choice. Washing towels, sheets, and pillowcases is a home care instruction that the nurse will offer to the client, as it prevents reinfection and transmission of bacteria or viruses. The client has conjunctivitis, which is inflammation of the conjunctiva or thin membrane that covers the white part of the eye and lines the eyelids. It can be caused by bacteria, viruses, allergies, or irritants.
B. Use antifungal drops 3 times a day
Reason: This is an incorrect choice. Using antifungal drops 3 times a day is not a home care instruction that the nurse will offer to the client, as it is not effective for conjunctivitis. Antifungal drops are used for fungal infections of the eye, which are rare and usually occur after trauma or surgery. The client may need antibiotic or antiviral drops, depending on the cause of conjunctivitis.
C. Schedule a sexually transmitted infection (STI/STD) exam
Reason: This is an incorrect choice. Scheduling a sexually transmitted infection (STI/STD) exam is not a home care instruction that the nurse will offer to the client, as it is not relevant for conjunctivitis. STIs can affect the eyes, but they usually cause different symptoms, such as redness, pain, or discharge from the urethra or vagina. The client may need to be tested for STIs if they have other risk factors or signs of infection.
D. Avoid going outside during daylight hours
Reason: This is an incorrect choice. Avoiding going outside during daylight hours is not a home care instruction that the nurse will offer to the client, as it is not necessary for conjunctivitis. The client may experience sensitivity to light, but they can wear sunglasses or avoid direct sunlight to protect their eyes. The client should also avoid rubbing or touching their eyes, wear glasses instead of contact lenses, and discard any eye makeup or cosmetics that may be contaminated.
Full Explanation
Choice A Reason: This is the correct choice. Washing towels, sheets, and pillowcases is a home care instruction that the nurse will offer to the client, as it prevents reinfection and transmission of bacteria or viruses. The client has conjunctivitis, which is inflammation of the conjunctiva or thin membrane that covers the white part of the eye and lines the eyelids. It can be caused by bacteria, viruses, allergies, or irritants.
Choice B Reason: This is an incorrect choice. Using antifungal drops 3 times a day is not a home care instruction that the nurse will offer to the client, as it is not effective for conjunctivitis. Antifungal drops are used for fungal infections of the eye, which are rare and usually occur after trauma or surgery. The client may need antibiotic or antiviral drops, depending on the cause of conjunctivitis.
Choice C Reason: This is an incorrect choice. Scheduling a sexually transmitted infection (STI/STD) exam is not a home care instruction that the nurse will offer to the client, as it is not relevant for conjunctivitis. STIs can affect the eyes, but they usually cause different symptoms, such as redness, pain, or discharge from the urethra or vagina. The client may need to be tested for STIs if they have other risk factors or signs of infection.
Choice D Reason: This is an incorrect choice. Avoiding going outside during daylight hours is not a home care instruction that the nurse will offer to the client, as it is not necessary for conjunctivitis. The client may experience sensitivity to light, but they can wear sunglasses or avoid direct sunlight to protect their eyes. The client should also avoid rubbing or touching their eyes, wear glasses instead of contact lenses, and discard any eye makeup or cosmetics that may be contaminated.
A nurse is preparing to review discharge instructions with a client who reports having hearing loss. Which of the following actions should the nurse plan to take?
A. Stand next to the client when speaking.
Choice A Reason: This is a correct choice. Standing next to the client when speaking is an action that the nurse should plan to take, as it helps the client hear better and see the nurse's facial expressions and lip movements. The nurse should also speak clearly and slowly, use simple words and sentences, and avoid covering their mouth.
B. Guide the client away from background noise.
Choice B Reason: This is a correct choice. Guiding the client away from background noise is an action that the nurse should plan to take, as it reduces distractions and interference with hearing. The nurse should also choose a well-lit and quiet place for communication and turn off any unnecessary devices or appliances.
C. Provide a copy of the instructions printed in Braille.
Choice C Reason: This is an incorrect choice. Providing a copy of the instructions printed in Braille is not an action that the nurse should plan to take, as it is not helpful for clients with hearing loss. Braille is a system of raised dots that represents letters and numbers for people who are blind or visually impaired. The nurse should provide a copy of the instructions printed in large font or use pictures or diagrams to supplement verbal information.
D. Repeat any phrases that the client misunderstands.
Choice D Reason: This is a correct choice. Repeating any phrases that the client misunderstands is an action that the nurse should plan to take, as it ensures comprehension and clarification of important information. The nurse should also ask open-ended questions, encourage feedback, and summarize key points at the end of the conversation.
Full Explanation
Choice A Reason: This is a correct choice. Standing next to the client when speaking is an action that the nurse should plan to take, as it helps the client hear better and see the nurse's facial expressions and lip movements. The nurse should also speak clearly and slowly, use simple words and sentences, and avoid covering their mouth.
Choice B Reason: This is a correct choice. Guiding the client away from background noise is an action that the nurse should plan to take, as it reduces distractions and interference with hearing. The nurse should also choose a well-lit and quiet place for communication and turn off any unnecessary devices or appliances.
Choice C Reason: This is an incorrect choice. Providing a copy of the instructions printed in Braille is not an action that the nurse should plan to take, as it is not helpful for clients with hearing loss. Braille is a system of raised dots that represents letters and numbers for people who are blind or visually impaired. The nurse should provide a copy of the instructions printed in large font or use pictures or diagrams to supplement verbal information.
Choice D Reason: This is a correct choice. Repeating any phrases that the client misunderstands is an action that the nurse should plan to take, as it ensures comprehension and clarification of important information. The nurse should also ask open-ended questions, encourage feedback, and summarize key points at the end of the conversation.