Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
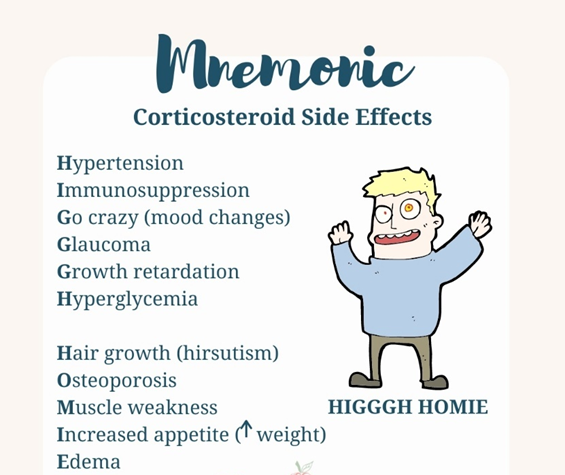
A nurse is planning care for a client who has multiple sclerosis and is receiving methylprednisolone. Which of the following adverse effects should the nurse anticipate? (Select all that apply.)
A. Bladder spasms
Bladder spasms are not commonly reported as adverse effects of methylprednisolone. However, bladder dysfunction can occur in individuals with multiple sclerosis due to the disease process itself, but it is not specifically related to corticosteroid therapy.
B. Hypotension
Hypotension is not a common adverse effect of methylprednisolone. In fact, corticosteroids can often lead to fluid retention and sodium retention, which can contribute to hypertension rather than hypotension.
C. Delayed wound healing
Corticosteroids can impair the body's ability to heal wounds by suppressing the inflammatory response and collagen synthesis. Therefore, clients receiving methylprednisolone may experience delayed wound healing, which can be problematic, especially in individuals with pre-existing wounds or undergoing surgical procedures.
D. Hirsutism
Hirsutism (excessive hair growth, especially in women) can occur with long-term corticosteroid use due to the effect of steroids on hair follicles. It is a possible adverse effect of methylprednisolone.
E. Hyperglycemia
Corticosteroids can increase blood glucose levels by promoting gluconeogenesis, reducing glucose uptake by tissues, and inducing insulin resistance. Clients receiving methylprednisolone may develop hyperglycemia, which can be particularly concerning for individuals with diabetes or those at risk of developing diabetes.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Medical Surgical Proctored Exam 1. Take the full exam now
Full Explanation
Choice A Reason:
Bladder spasms are not commonly reported as adverse effects of methylprednisolone. However, bladder dysfunction can occur in individuals with multiple sclerosis due to the disease process itself, but it is not specifically related to corticosteroid therapy.
Choice B Reason:
Hypotension is not a common adverse effect of methylprednisolone. In fact, corticosteroids can often lead to fluid retention and sodium retention, which can contribute to hypertension rather than hypotension.
Choice C Reason:
Delayed wound healing is correct. Corticosteroids can impair the body's ability to heal wounds by suppressing the inflammatory response and collagen synthesis. Therefore, clients receiving methylprednisolone may experience delayed wound healing, which can be problematic, especially in individuals with pre-existing wounds or undergoing surgical procedures.
Choice D Reason:
Hirsutism (excessive hair growth, especially in women) can occur with long-term corticosteroid use due to the effect of steroids on hair follicles. It is a possible adverse effect of methylprednisolone.
Choice E Reason:
Hyperglycemia is correct. Corticosteroids can increase blood glucose levels by promoting gluconeogenesis, reducing glucose uptake by tissues, and inducing insulin resistance. Clients receiving methylprednisolone may develop hyperglycemia, which can be particularly concerning for individuals with diabetes or those at risk of developing diabetes.
Similar Questions
A nurse in the emergency department is assessing a client who was brought in by a neighbor after falling down suddenly while walking. Which of the following assessments are the priority for the nurse to complete?(Select All that Apply.)
A. Muscle strength
Muscle strength is correct. Assessing muscle strength is essential to determine if there are any neurological deficits or weakness that could indicate a neurological condition or injury. Sudden falls can be indicative of various neurological issues, such as stroke or transient ischemic attack (TIA). Assessing muscle strength helps identify any motor impairments or weakness that could contribute to the fall.
B. Facial symmetry
Facial symmetry is correct. Assessing facial symmetry is crucial to identify any signs of facial droop, which could indicate a neurological deficit such as a stroke or Bell's palsy. Facial asymmetry may suggest damage to the facial nerve or other neurological issues.
C. Peripheral pulses
Peripheral pulses is incorrect. While assessing peripheral pulses is important for evaluating circulation, it may not be the priority assessment in this scenario where the client has suddenly fallen and may be experiencing neurological symptoms. Neurological deficits, such as weakness or changes in facial symmetry, vision, or speech, are more indicative of acute neurological issues like stroke or transient ischemic attack (TIA), which require immediate attention and intervention. In emergency situations, prioritizing assessments related to potential life-threatening conditions such as neurological deficits takes precedence over assessing peripheral pulses.
D. Vision changes
Vision changes is correct. Assessing for vision changes is important to identify any visual disturbances or deficits that could contribute to falls or indicate underlying neurological issues such as a stroke or transient ischemic attack (TIA). Visual disturbances may include blurriness, double vision, or loss of vision in one or both eyes.
E. Aphasia
Aphasia is incorrect. Assessing for aphasia, which is the inability to understand or express speech, is essential to identify any language deficits that could indicate a neurological condition such as a stroke. Aphasia may present as difficulty speaking, understanding language, or both.
Full Explanation
Choice A Reason:
Muscle strength is correct. Assessing muscle strength is essential to determine if there are any neurological deficits or weakness that could indicate a neurological condition or injury. Sudden falls can be indicative of various neurological issues, such as stroke or transient ischemic attack (TIA). Assessing muscle strength helps identify any motor impairments or weakness that could contribute to the fall.
Choice B Reason:
Facial symmetry is correct. Assessing facial symmetry is crucial to identify any signs of facial droop, which could indicate a neurological deficit such as a stroke or Bell's palsy. Facial asymmetry may suggest damage to the facial nerve or other neurological issues.
Choice C Reason:
Peripheral pulses is incorrect. While assessing peripheral pulses is important for evaluating circulation, it may not be the priority assessment in this scenario where the client has suddenly fallen and may be experiencing neurological symptoms. Neurological deficits, such as weakness or changes in facial symmetry, vision, or speech, are more indicative of acute neurological issues like stroke or transient ischemic attack (TIA), which require immediate attention and intervention. In emergency situations, prioritizing assessments related to potential life-threatening conditions such as neurological deficits takes precedence over assessing peripheral pulses.
Choice D Reason:
Vision changes is correct. Assessing for vision changes is important to identify any visual disturbances or deficits that could contribute to falls or indicate underlying neurological issues such as a stroke or transient ischemic attack (TIA). Visual disturbances may include blurriness, double vision, or loss of vision in one or both eyes.
Choice E Reason:
Aphasia is incorrect. Assessing for aphasia, which is the inability to understand or express speech, is essential to identify any language deficits that could indicate a neurological condition such as a stroke. Aphasia may present as difficulty speaking, understanding language, or both.
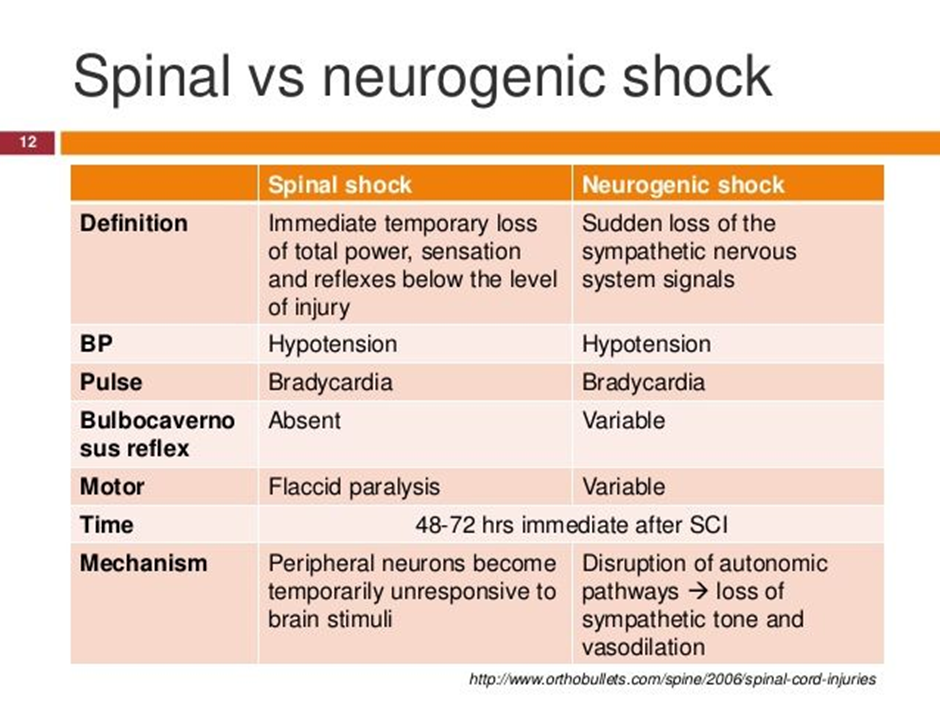
A nurse is planning care for a client who has neurogenic shock following a spinal cord injury. Which of the following provider prescriptions should the nurse anticipate? (Select all that apply.)
(Select All that Apply.)
A. Metoprolol
Metoprolol is incorrect. Metoprolol is a beta-blocker medication commonly used to treat conditions such as hypertension, angina, and heart failure. However, in the context of neurogenic shock following a spinal cord injury, the use of beta-blockers such as metoprolol is generally contraindicated. Beta-blockers antagonize the effects of sympathetic activation, leading to a reduction in heart rate and myocardial contractility, which can exacerbate hypotension and bradycardia, the hallmarks of neurogenic shock. Therefore, the nurse would not anticipate a prescription for metoprolol in the management of neurogenic shock.
B. Lactated Ringers intravenous fluid
Lactated Ringers intravenous fluid is correct. Fluid resuscitation with isotonic crystalloid solutions such as lactated Ringers is essential to restore intravascular volume and improve perfusion.
C. Furosemide
Furosemide is incorrect. Furosemide is a loop diuretic medication commonly used to treat conditions such as heart failure, edema, and hypertension by promoting diuresis and reducing fluid volume. However, in the context of neurogenic shock, the use of diuretics such as furosemide is generally not indicated unless there is concurrent volume overload. Neurogenic shock is characterized by hypotension due to vasodilation and decreased systemic vascular resistance, often leading to relative hypovolemia rather than volume overload. Therefore, administering furosemide could further decrease intravascular volume, exacerbating hypotension and compromising perfusion. As a result, the nurse would not anticipate a prescription for furosemide in the management of neurogenic shock.:
D. Dopamine
Dopamine is correct. Dopamine is a vasopressor medication that acts to increase vascular tone and blood pressure by stimulating alpha-adrenergic receptors. It is commonly used in the management of neurogenic shock to augment blood pressure.
E. Epinephrine
Epinephrine is correct. Epinephrine is a potent vasopressor that acts on both alpha and beta-adrenergic receptors, leading to vasoconstriction and increased cardiac output. It is used in the treatment of refractory hypotension in neurogenic shock.
Full Explanation
Choice A Reason:
Metoprolol is incorrect. Metoprolol is a beta-blocker medication commonly used to treat conditions such as hypertension, angina, and heart failure. However, in the context of neurogenic shock following a spinal cord injury, the use of beta-blockers such as metoprolol is generally contraindicated. Beta-blockers antagonize the effects of sympathetic activation, leading to a reduction in heart rate and myocardial contractility, which can exacerbate hypotension and bradycardia, the hallmarks of neurogenic shock. Therefore, the nurse would not anticipate a prescription for metoprolol in the management of neurogenic shock.
Choice B Reason:
Lactated Ringers intravenous fluid is correct. Fluid resuscitation with isotonic crystalloid solutions such as lactated Ringers is essential to restore intravascular volume and improve perfusion.
Choice C Reason:
Furosemide is incorrect. Furosemide is a loop diuretic medication commonly used to treat conditions such as heart failure, edema, and hypertension by promoting diuresis and reducing fluid volume. However, in the context of neurogenic shock, the use of diuretics such as furosemide is generally not indicated unless there is concurrent volume overload. Neurogenic shock is characterized by hypotension due to vasodilation and decreased systemic vascular resistance, often leading to relative hypovolemia rather than volume overload. Therefore, administering furosemide could further decrease intravascular volume, exacerbating hypotension and compromising perfusion. As a result, the nurse would not anticipate a prescription for furosemide in the management of neurogenic shock.:
Choice D Reason:
Dopamine is correct. Dopamine is a vasopressor medication that acts to increase vascular tone and blood pressure by stimulating alpha-adrenergic receptors. It is commonly used in the management of neurogenic shock to augment blood pressure.
Choice E Reason:
Epinephrine is correct. Epinephrine is a potent vasopressor that acts on both alpha and beta-adrenergic receptors, leading to vasoconstriction and increased cardiac output. It is used in the treatment of refractory hypotension in neurogenic shock.
A nurse is caring for a client who has headaches. In determining a diagnosis, which of the following precipitating factors is common in both tension-type headaches and cluster headaches?
A. Depression
Depression is incorrect. While depression can contribute to headaches in some individuals, it is more commonly associated with migraine headaches rather than tension-type headaches or cluster headaches. People with depression may experience changes in neurotransmitter levels and alterations in pain perception, which can exacerbate migraines. However, tension-type headaches and cluster headaches are generally less strongly associated with depression as a precipitating factor compared to migraines.
B. Smoking
Smoking is incorrect. Smoking can be a trigger for headaches in some individuals, particularly migraines, due to the vasoconstrictive effects of nicotine and other compounds in tobacco smoke. However, smoking is not universally recognized as a common precipitating factor for tension-type headaches or cluster headaches. While individuals with cluster headaches may have higher rates of smoking compared to the general population, it is not a factor commonly shared with tension-type headaches.
C. Poor posture
Poor posture is incorrect. Poor posture can contribute to muscle tension and cervical spine strain, which may trigger tension-type headaches. However, poor posture is not typically considered a precipitating factor specific to cluster headaches. While tension-type headaches may be exacerbated by poor posture, cluster headaches are characterized by severe, unilateral pain typically centered around the eye or temple, with associated autonomic symptoms such as tearing, nasal congestion, or ptosis.
D. Stress
Stress is correct. Stress is a well-established precipitating factor for both tension-type headaches and cluster headaches. Stress can lead to muscle tension and contraction, which are common triggers for tension-type headaches. Additionally, stress can also contribute to the onset or worsening of cluster headaches, although the exact mechanisms underlying this association are not fully understood. Therefore, stress is a common precipitating factor for both tension-type headaches and cluster headaches.
Full Explanation
Choice A Reason:
Depression is incorrect. While depression can contribute to headaches in some individuals, it is more commonly associated with migraine headaches rather than tension-type headaches or cluster headaches. People with depression may experience changes in neurotransmitter levels and alterations in pain perception, which can exacerbate migraines. However, tension-type headaches and cluster headaches are generally less strongly associated with depression as a precipitating factor compared to migraines.
Choice B Reason:
Smoking is incorrect. Smoking can be a trigger for headaches in some individuals, particularly migraines, due to the vasoconstrictive effects of nicotine and other compounds in tobacco smoke. However, smoking is not universally recognized as a common precipitating factor for tension-type headaches or cluster headaches. While individuals with cluster headaches may have higher rates of smoking compared to the general population, it is not a factor commonly shared with tension-type headaches.
Choice C Reason:
Poor posture is incorrect. Poor posture can contribute to muscle tension and cervical spine strain, which may trigger tension-type headaches. However, poor posture is not typically considered a precipitating factor specific to cluster headaches. While tension-type headaches may be exacerbated by poor posture, cluster headaches are characterized by severe, unilateral pain typically centered around the eye or temple, with associated autonomic symptoms such as tearing, nasal congestion, or ptosis.
Choice D Reason:
Stress is correct. Stress is a well-established precipitating factor for both tension-type headaches and cluster headaches. Stress can lead to muscle tension and contraction, which are common triggers for tension-type headaches. Additionally, stress can also contribute to the onset or worsening of cluster headaches, although the exact mechanisms underlying this association are not fully understood. Therefore, stress is a common precipitating factor for both tension-type headaches and cluster headaches.
