Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is preparing to administer amoxicillin 500 mg PO every 12 hr. The amount available is amoxicillin 250 mg/5 mL suspension. How many mL should the nurse administer?
(Round the answer to the nearest whole number. Use a leading zero if it applies. Do not use a trailing zero.)
This question is an excerpt from Nurse Dive's nursing test bank - ATI Med Surg Proctored Exam 1. Take the full exam now
Full Explanation
To calculate the amount of mL to administer, the nurse should use the following formula:
(mg ordered / mg available) x mL available = mL to administer
Substituting the values from the question, the nurse should do the following:
(500 mg / 250 mg) x 5 mL = 10 mL
Therefore, the nurse should administer 10 mL of amoxicillin suspension.

Similar Questions
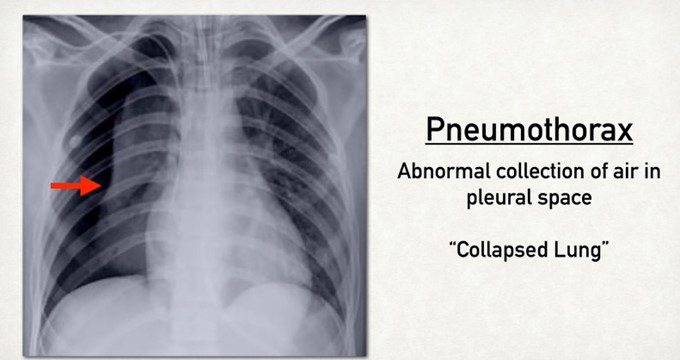
A nurse is monitoring a client who has a chest tube in place connected to wall suction due to a right-sided pneumothorax. The client complains of chest burning. Which of the following actions should the nurse take?
A. Increase the client's wall suction.
Increasing the client's wall suction is not advisable, as it can cause increased negative pressure in the pleural space and lead to tension pneumothorax. Increasing the wall suction does not affect the patency of the chest tube or the drainage of air or fluid from the lung. The nurse should maintain the wall suction at the prescribed level and monitor for any changes in the suction chamber.
B. Reposition the client.
Repositioning the client is the appropriate action for the nurse to take, as chest burning may indicate that the chest tube is kinked, twisted, or compressed, which can impair drainage and ventilation. The nurse should gently move the client to a different position and check that the chest tube is not bent or occluded by clothing, bedding, or furniture. The nurse should also ensure that there are no dependent loops or coils in the tubing and that it is secured to prevent dislodgment.
C. Clamp the client's chest tube.
Clamping the client's chest tube is not advisable, as it can cause air or fluid accumulation in the pleural space and lead to tension pneumothorax. Clamping the chest tube does not relieve chest burning or improve drainage or ventilation. The nurse should only clamp the chest tube for a brief period of time and under specific circumstances, such as changing the drainage system, assessing for an air leak, or preparing for chest tube removal.
D. Strip the client's chest tube.
Stripping the client's chest tube is not advisable, as it can cause increased negative pressure in the pleural space and lead to tissue damage or bleeding. Stripping the chest tube involves applying manual pressure along the tubing to force out any clots or debris that may obstruct drainage. However, this practice is not recommended, as it can cause more harm than good. The nurse should only milk the chest tube gently and intermittently if ordered by the provider and if there is evidence of obstruction.
Full Explanation
Repositioning the client is the appropriate action for the nurse to take, as chest burning may indicate that the chest tube is kinked, twisted, or compressed, which can impair drainage and ventilation. The nurse should gently move the client to a different position and check that the chest tube is not bent or occluded by clothing, bedding, or furniture. The nurse should also ensure that there are no dependent loops or coils in the tubing and that it is secured to prevent dislodgment.
a) Increasing the client's wall suction is not advisable, as it can cause increased negative pressure in the pleural space and lead to tension pneumothorax. Increasing the wall suction does not affect the patency of the chest tube or the drainage of air or fluid from the lung. The nurse should maintain the wall suction at the prescribed level and monitor for any changes in the suction chamber.
c) Clamping the client's chest tube is not advisable, as it can cause air or fluid accumulation in the pleural space and lead to tension pneumothorax. Clamping the chest tube does not relieve chest burning or improve drainage or ventilation. The nurse should only clamp the chest tube for a brief period of time and under specific circumstances, such as changing the drainage system, assessing for an air leak, or preparing for chest tube removal.
d) Stripping the client's chest tube is not advisable, as it can cause increased negative pressure in the pleural space and lead to tissue damage or bleeding. Stripping the chest tube involves applying manual pressure along the tubing to force out any clots or debris that may obstruct drainage. However, this practice is not recommended, as it can cause more harm than good. The nurse should only milk the chest tube gently and intermittently if ordered by the provider and if there is evidence of obstruction.
A nurse is caring for a client who has emphysema. Which of the following findings should the nurse expect to assess in this client? (Select all that apply)
A. Dyspnea
Dyspnea (shortness of breath) is a common symptom in emphysema due to the destruction of alveolar walls and the resulting reduction in surface area for gas exchange. As the disease progresses, the patient experiences increasing difficulty in breathing, especially during exertion or when the disease becomes more severe.
B. Barrel chest
A barrel chest is often seen in emphysema, as it results from hyperinflation of the lungs. The increased air trapping due to damaged alveoli causes the chest to expand and become rounded, leading to the characteristic "barrel chest" appearance. This happens because the lungs are constantly overinflated, and the chest wall becomes rigid and rounded as a result.
C. Deep respirations
While patients with emphysema may have increased respiratory effort or rate, deep respirations are not a hallmark feature. In fact, due to the damaged alveoli and reduced lung elasticity, breathing may become shallow and labored. Hyperventilation or rapid shallow breathing is more common, particularly during exertion, but deep respirations are not typically seen in emphysema.
D. Clubbing of the fingers
Clubbing of the fingers can occur in chronic respiratory conditions like emphysema due to prolonged hypoxia (low oxygen levels in the blood). This is a compensatory mechanism that involves changes in the nails and fingers. The tips of the fingers become rounded and bulbous over time, and this is commonly associated with long-standing pulmonary diseases.
E. Bradycardia
Bradycardia (slow heart rate) is not typically associated with emphysema. In fact, patients with emphysema often experience tachycardia (increased heart rate), particularly in response to hypoxia and the body's attempt to compensate for the reduced oxygen supply. Bradycardia is not a typical finding in this condition.
Full Explanation
A. Dyspnea:
Dyspnea (shortness of breath) is a common symptom in emphysema due to the destruction of alveolar walls and the resulting reduction in surface area for gas exchange. As the disease progresses, the patient experiences increasing difficulty in breathing, especially during exertion or when the disease becomes more severe.
B. Barrel chest:
A barrel chest is often seen in emphysema, as it results from hyperinflation of the lungs. The increased air trapping due to damaged alveoli causes the chest to expand and become rounded, leading to the characteristic "barrel chest" appearance. This happens because the lungs are constantly overinflated, and the chest wall becomes rigid and rounded as a result.
D. Clubbing of the fingers:
Clubbing of the fingers can occur in chronic respiratory conditions like emphysema due to prolonged hypoxia (low oxygen levels in the blood). This is a compensatory mechanism that involves changes in the nails and fingers. The tips of the fingers become rounded and bulbous over time, and this is commonly associated with long-standing pulmonary diseases.
A nurse is providing discharge teaching to a client who has a new prescription for home oxygen therapy via a nasal cannula. Which of the following should the nurse include in the teaching? (Select all that apply)
A. Post no smoking signs in a prominent location in the home.
These are important safety and comfort measures for a client who uses home oxygen therapy via a nasal cannula.
B. Verify the oxygen flow rate every other day.
Verify the oxygen flow rate every other day. This is not frequent enough, as the flow rate should be checked at least daily and whenever the client feels short of breath or has changes in vital signs.
C. Check the tops of the ears for skin breakdown.
These are important safety and comfort measures for a client who uses home oxygen therapy via a nasal cannula.
D. Apply petroleum ointment to nares if they become dry and irritated.
Apply petroleum ointment to nares if they become dry and irritated. This is not recommended, as petroleum products can ignite in the presence of oxygen and cause burns or fire. A water-based lubricant should be used instead.
E. Check the cannula position on a regular basis.
These are important safety and comfort measures for a client who uses home oxygen therapy via a nasal cannula.
Full Explanation
These are important safety and comfort measures for a client who uses home oxygen therapy via a nasal cannula.
The other options are not correct because:
b. Verify the oxygen flow rate every other day. This is not frequent enough, as the flow rate should be checked at least daily and whenever the client feels short of breath or has changes in vital signs.
d. Apply petroleum ointment to nares if they become dry and irritated. This is not recommended, as petroleum products can ignite in the presence of oxygen and cause burns or fire. A water-based lubricant should be used instead.