Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
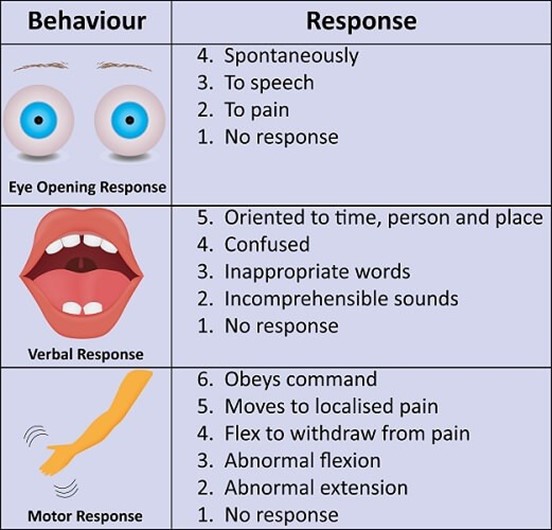
A nurse is receiving a transfer report for a client who has a head injury. The client has a Glasgow Coma Scale (GCS) score of 3 for eye opening, 5 for best verbal response, and 5 for best motor response. Which of the following is an appropriate conclusion based on this data?
A. The client is unconscious.
B. The client is unable to make vocal sound.
C. The client can follow simple motor commands.
D. The client opens his eyes when spoken to.
An appropriate conclusion based on this data is that the client opens his eyes when spoken to. A GCS score of 3 for eye opening indicates that the client opens his eyes in response to voice. The client is not unconscious, as a GCS score of 3 for eye opening indicates that the client is able to open his eyes in response to voice. The client is not unable to make vocal sound, as a GCS score of 5 for best verbal response indicates that the client is able to make vocal sounds. The client may or may not be able to follow simple motor commands, as a GCS score of 5 for best motor response indicates that the client is able to localize pain.
This question is an excerpt from Nurse Dive's nursing test bank - ATI Custom MS Nurse Proctored Exam. Take the full exam now
Full Explanation
An appropriate conclusion based on this data is that the client opens his eyes when spoken to. A GCS score of 3 for eye opening indicates that the client opens his eyes in response to voice.
The client is not unconscious, as a GCS score of 3 for eye opening indicates that the client is able to open his eyes in response to voice. The client is not unable to make vocal sound, as a GCS score of 5 for best verbal response indicates that the client is able to make vocal sounds. The client may or may not be able to follow simple motor commands, as a GCS score of 5 for best motor response indicates that the client is able to localize pain.
Similar Questions
A nurse is assisting a client who is postoperative following a total hip arthroplasty into a supine position. Which of the following actions is appropriate to prevent hip dislocation?
A. Place a trochanter roll against the thigh.
B. Place a sandbag to the lateral calf.
C. Place a wedge pillow between the legs.
An appropriate action to prevent hip dislocation in a client who is postoperative following a total hip arthroplasty is to place a wedge pillow between the legs. This helps to maintain proper alignment and prevent the legs from crossing or adducting, which can cause hip dislocation. Placing a trochanter roll against the thigh, placing a sandbag on the lateral calf, and placing a footboard on the bed are not appropriate actions to prevent hip dislocation in this situation. A trochanter roll is used to prevent the external rotation of the hip. A sandbag to the lateral calf can help prevent foot drop. A footboard can help prevent plantar flexion contractures.
D. Place a footboard on the bed.
Full Explanation
An appropriate action to prevent hip dislocation in a client who is postoperative following a total hip arthroplasty is to place a wedge pillow between the legs. This helps to maintain proper alignment and prevent the legs from crossing or adducting, which can cause hip dislocation.
Placing a trochanter roll against the thigh, placing a sandbag on the lateral calf, and placing a footboard on the bed are not appropriate actions to prevent hip dislocation in this situation. A trochanter roll is used to prevent the external rotation of the hip. A sandbag to the lateral calf can help prevent foot drop. A footboard can help prevent plantar flexion contractures.
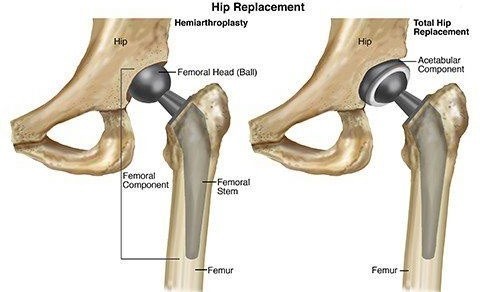
A nurse is caring for a client who is postoperative following a right total hip arthroplasty. In which of the following positions should the nurse place the client's right leg?
A. Internal rotation
B. Abduction
The nurse should place the client's right leg in abduction following a right total hip arthroplasty. Abduction means moving the leg away from the midline of the body. This position helps to prevent hip dislocation by keeping the hip joint in proper alignment. Internal rotation, adduction, and external rotation are not appropriate positions for the client's right leg following a right total hip arthroplasty. Internal rotation means turning the leg inward towards the midline of the body. Adduction means moving the leg towards the midline of the body. External rotation means turning the leg outward away from the midline of the body. These positions can increase the risk of hip dislocation.
C. Adduction
D. External rotation
Full Explanation
The nurse should place the client's right leg in abduction following a right total hip arthroplasty. Abduction means moving the leg away from the midline of the body. This position helps to prevent hip dislocation by keeping the hip joint in proper alignment.
Internal rotation, adduction, and external rotation are not appropriate positions for the client's right leg following a right total hip arthroplasty. Internal rotation means turning the leg inward towards the midline of the body. Adduction means moving the leg towards the midline of the body. External rotation means turning the leg outward away from the midline of the body. These positions can increase the risk of hip dislocation.
A nurse in a long-term care facility finds an older adult client lying on the floor next to the bed. Which of the following actions should the nurse take?
A. Check the client for injuries.
The first action the nurse should take is to check the client for injuries. The nurse should assess the client for any signs of injury or trauma and provide appropriate care as needed. Obtaining a prescription for medication to sedate the client, calling the family and asking them to make arrangements for someone to sit with the client, assisting the client back into bed and applying restraints are not appropriate initial actions for the nurse to take in this situation. These actions may be considered after the client has been assessed for injuries and their immediate needs have been addressed.
B. Obtain a prescription for medication to sedate the client.
C. Call the family and ask them to make arrangements for someone to sit with the client.
D. Assist the client back into bed and apply restraints.
Full Explanation
The first action the nurse should take is to check the client for injuries. The nurse should assess the client for any signs of injury or trauma and provide appropriate care as needed.
Obtaining a prescription for medication to sedate the client, calling the family and asking them to make arrangements for someone to sit with the client, and assisting the client back into bed and applying restraints are not appropriate initial actions for the nurse to take in this situation. These actions may be considered after the client has been assessed for injuries and their immediate needs have been addressed.