Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is reinforcing teaching with a client who is at 16 weeks of gestation and has a prescription for ferrous sulfate to treat iron-deficiency anemia. Which of the following recommendations should the nurse make to improve the absorption of the medication?
A. "Increase your dietary fiber intake."
While increasing dietary fiber can help with constipation, a common side effect of iron supplements, it does not directly improve the absorption of the medication
B. "Eliminate berries and citrus fruits from your diet."
Berries and citrus fruits, on the other hand, are good sources of vitamin C, which can actually enhance iron absorption. Therefore, eliminating them from the diet would not be beneficial for improving iron absorption.
C. "Avoid drinking milk with the iron supplement.:
The recommendation the nurse should make to improve the absorption of the iron supplement (ferrous sulfate) is to avoid drinking milk with the medication. Calcium in milk can interfere with the absorption of iron, so it is best to separate the consumption of these two substances.
D. "Take the iron supplement with green tea."
Green tea contains compounds called tannins, which can interfere with iron absorption. Therefore, it is not recommended to take iron supplements with green tea.
This question is an excerpt from Nurse Dive's nursing test bank - PN Comprehensive Predictor PN 2020 Proctored Exam. Take the full exam now
Full Explanation
A. While increasing dietary fiber can help with constipation, a common side effect of iron supplements, it does not directly improve the absorption of the medication
B. Berries and citrus fruits, on the other hand, are good sources of vitamin C, which can actually enhance iron absorption. Therefore, eliminating them from the diet would not be beneficial for improving iron absorption.
C. The recommendation the nurse should make to improve the absorption of the iron supplement (ferrous sulfate) is to avoid drinking milk with the medication. Calcium in milk can interfere with the absorption of iron, so it is best to separate the consumption of these two substances.
D. Green tea contains compounds called tannins, which can interfere with iron absorption. Therefore, it is not recommended to take iron supplements with green tea.
Similar Questions
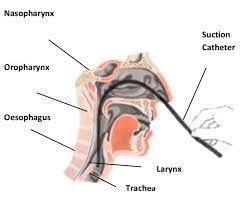
A nurse is performing nasopharyngeal suctioning for an adult client. Which of the following techniques should the nurse use?
A. Apply intermittent suction for 30 seconds.
The nurse should also apply intermittent suction for no longer than 15 seconds to prevent hypoxia and damage to the mucosal lining. Suctioning for an extended period can cause discomfort and harm to the client.
B. Insert the catheter 10 cm (4 in).
The distance that the nasopharyngeal catheter should be inserted varies from person to person and therefore 10 cm is not standard.
C. Apply suction while inserting the catheter.
During nasopharyngeal suctioning, the nurse should apply suction intermittently while withdrawing the catheter, not during insertion. Applying suction during insertion can cause tissue damage and increase the risk of trauma.
D. Wait 1 min between suctioning attempts.
Waiting 1 minute between suctioning attempts allows the client to recover and ensures that the procedure is not overly invasive. It also helps to prevent the client from becoming hypoxic.
Full Explanation
Waiting 1 minute between suctioning attempts allows the client to recover and ensures that the procedure is not overly invasive. It also helps to prevent the client from becoming hypoxic.
The distance that the nasopharyngeal catheter should be inserted varies from person to person and therefore 10 cm is not standard.
During nasopharyngeal suctioning, the nurse should apply suction intermittently while withdrawing the catheter, not during insertion. Applying suction during insertion can cause tissue damage and increase the risk of trauma.
The nurse should also apply intermittent suction for no longer than 15 seconds to prevent hypoxia and damage to the mucosal lining. Suctioning for an extended period can cause discomfort and harm to the client.
A nurse is monitoring a client who is postoperative. Which of the following actions should the nurse take when collecting data about the client's respirations?
A. Place the client in a supine position.
Placing the client in a supine position may not be necessary for assessing respirations, as it is primarily focused on observing the chest movements.
B. Observe the movements of the client's chest wall.
To accurately assess the client's respirations, the nurse should observe the movements of the client's chest wall. This can be done by visually inspecting the rise and fall of the chest or by placing a hand on the client's chest to feel the movements. This allows the nurse to assess the depth, rhythm, and effort of the client's breathing. I
C. Inform the client when beginning to observe his respirations.
It is important to observe the client's respirations without informing them, as this may cause the client to alter their breathing pattern consciously.
D. Count the client's respirations for 15 seconds.
Counting the client's respirations for a full minute (rather than 15 seconds) provides a more accurate measurement.
Full Explanation
To accurately assess the client's respirations, the nurse should observe the movements of the client's chest wall. This can be done by visually inspecting the rise and fall of the chest or by placing a hand on the client's chest to feel the movements. This allows the nurse to assess the depth, rhythm, and effort of the client's breathing. I
It is important to observe the client's respirations without informing them, as this may cause the client to alter their breathing pattern consciously.
Counting the client's respirations for a full minute (rather than 15 seconds) provides a more accurate measurement.
Placing the client in a supine position may not be necessary for assessing respirations, as it is primarily focused on observing the chest movements.

A nurse is assisting with monitoring a client who is receiving a unit of packed RBCs. Which of the following findings indicates the client is experiencing a hemolytic transfusion reaction?
A. Temperature 38.8° C (101.8° F)
A temperature of 38.8° C (101.8° F) is indicative of a fever, which is a common symptom of a hemolytic transfusion reaction. During such a reaction, the immune system attacks the transfused red blood cells, leading to their destruction and the release of substances that can cause a rise in body temperature.
B. Straw-colored urine
Straw-colored urine is not typically associated with a hemolytic transfusion reaction. Hemolytic reactions often result in darker urine due to the presence of free hemoglobin released from destroyed red blood cells.
C. Apical pulse rate 58/min
An apical pulse rate of 58/min is considered bradycardia if it is lower than the normal resting heart rate for adults, which ranges from 60 to 100 beats per minute. Bradycardia is not a direct indicator of a hemolytic transfusion reaction.
D. Blood pressure 158/92 mm Hg
Elevated blood pressure, such as 158/92 mm Hg, can be a sign of various conditions but is not a specific indicator of a hemolytic transfusion reaction. The symptoms of such a reaction are more directly related to the destruction of red blood cells and the body’s response to it.
Full Explanation
The correct answer is: a. Temperature 38.8° C (101.8° F)
Title: Choice A reason: A temperature of 38.8° C (101.8° F) is indicative of a fever, which is a common symptom of a hemolytic transfusion reaction. During such a reaction, the immune system attacks the transfused red blood cells, leading to their destruction and the release of substances that can cause a rise in body temperature.
Title: Choice B reason: Straw-colored urine is not typically associated with a hemolytic transfusion reaction. Hemolytic reactions often result in darker urine due to the presence of free hemoglobin released from destroyed red blood cells.
Title: Choice C reason: An apical pulse rate of 58/min is considered bradycardia if it is lower than the normal resting heart rate for adults, which ranges from 60 to 100 beats per minute. Bradycardia is not a direct indicator of a hemolytic transfusion reaction.
Title: Choice D reason: Elevated blood pressure, such as 158/92 mm Hg, can be a sign of various conditions but is not a specific indicator of a hemolytic transfusion reaction. The symptoms of such a reaction are more directly related to the destruction of red blood cells and the body’s response to it.