Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is reinforcing teaching with an adolescent who has a new prescription for cefazolin.
For which of the following findings should the nurse instruct the adolescent to monitor and report to the provider?
A. Constipation
A. Constipation: Constipation is not a typical adverse effect of cefazolin. Antibiotics generally cause gastrointestinal symptoms like diarrhea rather than constipation, so this is not a primary concern with cefazolin therapy.
B. Elevated skin patches
B. Elevated skin patches: Elevated skin patches may indicate an allergic reaction, such as hives or a rash, which can be a serious side effect of cefazolin. Allergic reactions to antibiotics can escalate quickly and may require immediate medical attention. Monitoring for and reporting any skin changes is important to prevent potential complications.
C. Ringing in the ears
C. Ringing in the ears: Tinnitus (ringing in the ears) is not commonly associated with cefazolin. This symptom is more frequently associated with certain other antibiotics, such as aminoglycosides, but is not a primary concern with cefazolin use.
D. Depression
D. Depression: Depression is not a known side effect of cefazolin. While mood changes may be seen with some medications, cefazolin’s primary side effects are related to hypersensitivity reactions and gastrointestinal symptoms.
E. None
None
F. None
None
This question is an excerpt from Nurse Dive's nursing test bank - VATI PN Comprehensive Predictor 2020 Proctored Exam. Take the full exam now
Full Explanation
Answer: B. Elevated skin patches
Rationale:
A. Constipation:
Constipation is not a typical adverse effect of cefazolin. Antibiotics generally cause gastrointestinal symptoms like diarrhea rather than constipation, so this is not a primary concern with cefazolin therapy.
B. Elevated skin patches:
Elevated skin patches may indicate an allergic reaction, such as hives or a rash, which can be a serious side effect of cefazolin. Allergic reactions to antibiotics can escalate quickly and may require immediate medical attention. Monitoring for and reporting any skin changes is important to prevent potential complications.
C. Ringing in the ears:
Tinnitus (ringing in the ears) is not commonly associated with cefazolin. This symptom is more frequently associated with certain other antibiotics, such as aminoglycosides, but is not a primary concern with cefazolin use.
D. Depression:
Depression is not a known side effect of cefazolin. While mood changes may be seen with some medications, cefazolin’s primary side effects are related to hypersensitivity reactions and gastrointestinal symptoms.
Similar Questions
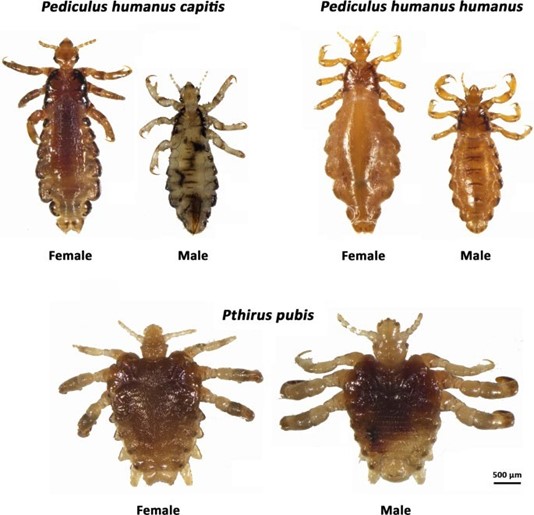
A nurse in a provider's office is reinforcing teaching with the parents of a school-age child who has an active case of Pediculosis humanus capitis. Which of the following should the nurse include in the teaching?
A. Apply a topical corticosteroid ointment to the scalp.
A) Apply a topical corticosteroid ointment to the scalp: Corticosteroids are not indicated for the treatment of Pediculosis capitis (head lice). The treatment focuses on eliminating the lice and nits, typically through pediculicide medications like permethrin or ivermectin. Corticosteroids are used to reduce inflammation and itching, but they do not kill the lice or their eggs.
B. Soak hair brushes and combs in soapy water.
B) Soak hair brushes and combs in soapy water: Soaking hair brushes and combs in soapy water alone is not sufficient to kill lice. Items such as hair brushes should be soaked in hot water (130°F or higher) for at least 5-10 minutes to ensure any lice or nits present are killed. This is a critical step to prevent reinfestation.
C. Wash the bed linens in hot water
C) Wash the bed linens in hot water: Washing bed linens in hot water (130°F or higher) is essential to eliminate lice and nits that may have transferred onto bedding. This prevents the spread and recurrence of lice. Items that cannot be washed should be sealed in a plastic bag for 2 weeks to kill the lice.
D. Clean the child's toys with 1:10 bleach solution.
D) Clean the child's toys with a 1:10 bleach solution: Lice are spread through direct contact and cannot live on inanimate objects for long periods. Cleaning toys with bleach is unnecessary for lice removal and can be harmful to the toys or the child if not properly rinsed.
E. None
None
F. None
None
Full Explanation
Answer: C
Rationale:
A) Apply a topical corticosteroid ointment to the scalp: Corticosteroids are not indicated for the treatment of Pediculosis capitis (head lice). The treatment focuses on eliminating the lice and nits, typically through pediculicide medications like permethrin or ivermectin. Corticosteroids are used to reduce inflammation and itching, but they do not kill the lice or their eggs.
B) Soak hair brushes and combs in soapy water: Soaking hair brushes and combs in soapy water alone is not sufficient to kill lice. Items such as hair brushes should be soaked in hot water (130°F or higher) for at least 5-10 minutes to ensure any lice or nits present are killed. This is a critical step to prevent reinfestation.
C) Wash the bed linens in hot water: Washing bed linens in hot water (130°F or higher) is essential to eliminate lice and nits that may have transferred onto bedding. This prevents the spread and recurrence of lice. Items that cannot be washed should be sealed in a plastic bag for 2 weeks to kill the lice.
D) Clean the child's toys with a 1:10 bleach solution: Lice are spread through direct contact and cannot live on inanimate objects for long periods. Cleaning toys with bleach is unnecessary for lice removal and can be harmful to the toys or the child if not properly rinsed.
A nurse is assisting with planning care for a newly admited client who has anorexia nervosa. Which of the following interventions should the nurse recommend to include in the plan of care?
A. Encourage the client to gain 2.3 kg (5 lb) per week.
A weight gain goal of 0.5 to 1 kg (1 to 2 lb) per week is considered safe and realistic. Gaining 2.3 kg (5 lb) weekly is too aggressive and may cause physical and psychological stress for the client.
B. Monitor the client for 15 min after meals
Clients with anorexia nervosa are at risk for purging behaviors. Monitoring for only 15 minutes is insufficient. A 60-minute post-meal observation period is more appropriate to deter vomiting or excessive exercise.
C. Weigh the client each morning after voiding
Daily weights, taken at the same time each morning after voiding and before eating, provide consistent and accurate data to monitor progress and detect manipulation or fluid shifts.
D. Reinforce teaching about healthy eating during meals
Reinforcing education during meals can increase the client’s anxiety and resistance to eating. Teaching is best done separately from mealtimes to avoid associating eating with stress.
Full Explanation
Answer: C. Weigh the client each morning after voiding
Rationale:
A. Encourage the client to gain 2.3 kg (5 lb) per week:
A weight gain goal of 0.5 to 1 kg (1 to 2 lb) per week is considered safe and realistic. Gaining 2.3 kg (5 lb) weekly is too aggressive and may cause physical and psychological stress for the client.
B. Monitor the client for 15 min after meals:
Clients with anorexia nervosa are at risk for purging behaviors. Monitoring for only 15 minutes is insufficient. A 60-minute post-meal observation period is more appropriate to deter vomiting or excessive exercise.
C. Weigh the client each morning after voiding:
Daily weights, taken at the same time each morning after voiding and before eating, provide consistent and accurate data to monitor progress and detect manipulation or fluid shifts.
D. Reinforce teaching about healthy eating during meals:
Reinforcing education during meals can increase the client’s anxiety and resistance to eating. Teaching is best done separately from mealtimes to avoid associating eating with stress.
A nurse is collecting data from the guardian of a toddler during a well-child visit. The guardian expresses concern to the nurse because his child has a poor appetite, but drinks a quart of milk each day.
The nurse should identify that this practice places the toddler at risk for which of the following conditions?
A. Celiac disease
Celiac disease is an autoimmune disorder triggered by the ingestion of gluten-containing foods, not specifically related to milk consumption.
B. Lactose intolerance
Lactose intolerance is a condition where the body has difficulty digesting lactose, the sugar found in milk, but it does not necessarily relate to the amount of milk consumed.
C. Acute renal failure
Acute renal failure is a severe condition involving the sudden loss of kidney function and is not directly associated with milk consumption.
D. Iron-deficiency anemia
Excessive milk consumption in toddlers can put them at risk for iron-deficiency anemia. Milk is a poor source of iron, and when a child consumes a large amount of milk, it can displace other iron-rich foods from their diet. Iron is essential for the production of hemoglobin, which carries oxygen in the blood. When a child does not consume enough iron, it can lead to iron-deficiency anemia, which can result in symptoms such as fatigue, pale skin, weakness, and poor appetite.