Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is reviewing a client’s laboratory results prior to administering the client’s medications. The nurse notes that the client’s lithium level is 2.0 mEq/L.
Which of the following findings should the nurse expect?
A. Muscle irritability.
. A client with a lithium level of
B. Constipation.
Choice B is wrong because constipation is not a sign of lithium toxicity, but rather a possible side effect of lithium therapy at lower doses.
C. Hypoglycemia.
Choice C is wrong because hypoglycemia is not a sign of lithium toxicity, but rather a possible complication of diabetes or other conditions that affect blood sugar levels.
D. Increased BP.
Choice D is wrong because increased blood pressure is not a sign of lithium toxicity, but rather a possible risk factor for cardiovascular disease or other conditions that affect blood vessels.
This question is an excerpt from Nurse Dive's nursing test bank - ATI PN Capstone Proctored Comprehensive Assessment 2020 B. Take the full exam now
Full Explanation
Muscle irritability. A client with a lithium level of
2.0 mEq/L has severe lithium toxicity, which can cause muscle irritability, tremors, seizures, and other neurological symptoms. The normal therapeutic range for lithium is 0.8-1.2 mEq/L.
Choice B is wrong because constipation is not a sign of lithium toxicity, but rather a possible side effect of lithium therapy at lower doses.
Choice C is wrong because hypoglycemia is not a sign of lithium toxicity, but rather a possible complication of diabetes or other conditions that affect blood sugar levels.
Choice D is wrong because increased blood pressure is not a sign of lithium toxicity, but rather a possible risk factor for cardiovascular disease or other conditions that affect blood vessels.
Similar Questions
A nurse is collecting data from a client who is at 29 weeks of gestation.
Which of the following findings should the nurse identify as a potential indication of a prenatal complication?
A. Leg cramps.
Choice A is wrong because leg cramps are a common discomfort during pregnancy and are not usually a sign of a complication.
B. Ptyalism.
Choice B is wrong because ptyalism, or excessive salivation, is a normal physiological change during pregnancy and does not indicate a problem.
C. Blurred vision.
This can be a sign of preeclampsia, a serious complication of pregnancy that causes high blood pressure and proteinuria.
D. Melasma.
Choice D is wrong because melasma, or darkening of the skin on the face, is also a normal physiological change during pregnancy and does not pose a risk to the mother or the fetus.
Full Explanation
This can be a sign of preeclampsia, a serious complication of pregnancy that causes high blood pressure and proteinuria.
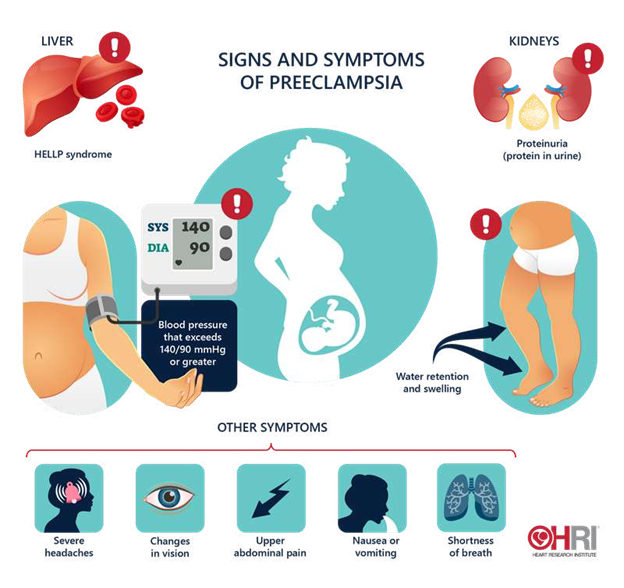
The nurse should report this finding to the provider and monitor the client’s blood pressure, urine protein, and reflexes.
Choice A is wrong because leg cramps are a common discomfort during pregnancy and are not usually a sign of a complication.
Choice B is wrong because ptyalism, or excessive salivation, is a normal physiological change during pregnancy and does not indicate a problem.
Choice D is wrong because melasma, or darkening of the skin on the face, is also a normal physiological change during pregnancy and does not pose a risk to the mother or the fetus.
A nurse is reinforcing teaching with a newly licensed nurse about discharge planning.
Which of the following statements by the newly licensed nurse indicates an understanding of the teaching?
A. The nurse is responsible for providing a written prescription for a client home care referral.
Choice A is wrong because the nurse is not responsible for providing a written prescription for a client home care referral. This is the role of the provider or another authorised prescriber.
B. The nurse should begin discharge planning upon the client’s admission.
The nurse should begin discharge planning upon the client’s admission. This is because discharge planning is a key aspect of effective care that reduces the length of stay, emergency readmissions and pressure on hospital beds. Discharge planning involves considering what support might be required by the client in the community, referring the client to these services, and liaising with these services to manage the client’s discharge.
C. A home hazard appraisal includes an assessment of the client’s financial resources.
Choice C is wrong because a home hazard appraisal does not include an assessment of the client’s financial resources. A home hazard appraisal is an evaluation of the safety and accessibility of the client’s home environment.
D. A medication reconciliation is required 24 hours prior to the client’s discharge.
Choice D is wrong because a medication reconciliation is not required 24 hours prior to the client’s discharge. A medication reconciliation is a process of comparing the medications a client is taking with those prescribed for them to avoid errors or discrepancies. A medication reconciliation should be done at every transition of care, including admission, transfer and discharge.
Full Explanation
The nurse should begin discharge planning upon the client’s admission. This is because discharge planning is a key aspect of effective care that reduces the length of stay, emergency readmissions and pressure on hospital beds. Discharge planning involves considering what support might be required by the client in the community, referring the client to these services, and liaising with these services to manage the client’s discharge.
Choice A is wrong because the nurse is not responsible for providing a written prescription for a client home care referral. This is the role of the provider or another authorised prescriber.
Choice C is wrong because a home hazard appraisal does not include an assessment of the client’s financial resources. A home hazard appraisal is an evaluation of the safety and accessibility of the client’s home environment.
Choice D is wrong because a medication reconciliation is not required 24 hours prior to the client’s discharge. A medication reconciliation is a process of comparing the medications a client is taking with those prescribed for them to avoid errors or discrepancies. A medication reconciliation should be done at every transition of care, including admission, transfer and discharge.
A nurse is using an interpreter to communicate with a client who speaks a different language than the nurse.
Which of the following actions should the nurse take?
A. Avoid asking the client personal questions.
Choice A is wrong because avoiding asking the client personal questions can hinder rapport building and prevent the nurse from obtaining important information about the client’s health and needs.
B. Observe the client’s body language during the conversation.
Observe the client’s body language during the conversation. This action will help the nurse to assess the client’s nonverbal cues and emotions, which can enhance communication and understanding. The nurse should also determine the client’s understanding several times during the conversation and use lay terms if possible.
C. Maintain eye contact with the interpreter when asking questions.
Choice C is wrong because maintaining eye contact with the interpreter when asking questions can show disrespect and disinterest to the client and his family. The nurse should look at the client and his family when asking questions, not at the interpreter.
D. Include medical terminology when discussing the client’s condition.
Choice D is wrong because including medical terminology when discussing the client’s condition can confuse the client and his family and create barriers to communication. The nurse should use simple and clear language that the client and his family can understand.
Full Explanation
Observe the client’s body language during the conversation. This action will help the nurse to assess the client’s nonverbal cues and emotions, which can enhance communication and understanding. The nurse should also determine the client’s understanding several times during the conversation and use lay terms if possible.
Choice A is wrong because avoiding asking the client personal questions can hinder rapport building and prevent the nurse from obtaining important information about the client’s health and needs.
Choice C is wrong because maintaining eye contact with the interpreter when asking questions can show disrespect and disinterest to the client and his family. The nurse should look at the client and his family when asking questions, not at the interpreter.
Choice D is wrong because including medical terminology when discussing the client’s condition can confuse the client and his family and create barriers to communication. The nurse should use simple and clear language that the client and his family can understand.