Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
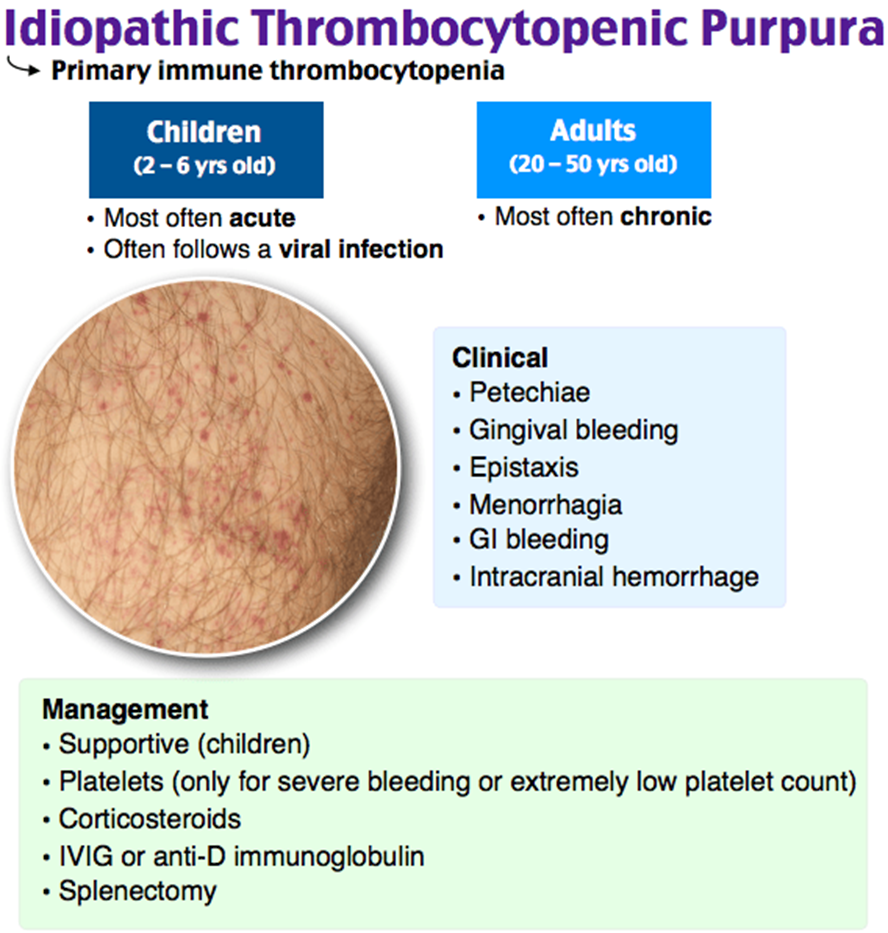
A nurse is reviewing the laboratory findings for a client who has idiopathic thrombocytopenic purpura (ITP). Which of the following findings should the nurse expect to be decreased?
A. RBC
RBC (Red Blood Cells): ITP primarily affects platelet levels, not red blood cells. Therefore, red blood cell counts are not typically decreased in ITP.
B. Platelets
Platelets: This is the correct answer. ITP is characterized by a low platelet count due to immune-mediated destruction of platelets. A decreased platelet count can lead to an increased risk of bleeding.
C. Granulocytes
Granulocytes: While ITP primarily affects platelets, it does not have a direct impact on granulocyte counts. Granulocytes are a type of white blood cell.
D. WBC
WBC (White Blood Cells): ITP primarily affects platelets, not white blood cells. Therefore, white blood cell counts are not typically decreased in ITP.
This question is an excerpt from Nurse Dive's nursing test bank - Smith Chason Los Angeles ATI Med Surg Proctored Exam 2. Take the full exam now
Full Explanation
A. RBC (Red Blood Cells): ITP primarily affects platelet levels, not red blood cells. Therefore, red blood cell counts are not typically decreased in ITP.
B. Platelets: This is the correct answer. ITP is characterized by a low platelet count due to immune-mediated destruction of platelets. A decreased platelet count can lead to an increased risk of bleeding.
C. Granulocytes: While ITP primarily affects platelets, it does not have a direct impact on granulocyte counts. Granulocytes are a type of white blood cell.
D. WBC (White Blood Cells): ITP primarily affects platelets, not white blood cells. Therefore, white blood cell counts are not typically decreased in ITP.
Similar Questions
A nurse is reviewing blood pressure classifications with a group of nurses at an in-service meeting. Which of the following should the nurse include as a risk factor for the development of hypertension?
A. High-density lipoprotein (HDL) level of 70 mg/dL
High-density lipoprotein (HDL) level of 70 mg/dL: Having a high HDL level is generally considered a protective factor against cardiovascular disease, including hypertension.
B. A diet high in potassium
A diet high in potassium: A diet high in potassium is often associated with a lower risk of hypertension. Potassium helps balance sodium levels and supports healthy blood pressure.
C. Obstructive sleep apnea (OSA)
Obstructive sleep apnea (OSA): This is the correct answer. Obstructive sleep apnea is a known risk factor for hypertension. The repeated episodes of interrupted breathing during sleep can contribute to increased blood pressure.
D. Taking benazepril
Taking benazepril: Benazepril is an angiotensin-converting enzyme (ACE) inhibitor commonly used to treat hypertension. While it is used to manage high blood pressure, taking the medication itself is not a risk factor for developing hypertension.
Full Explanation
A. High-density lipoprotein (HDL) level of 70 mg/dL: Having a high HDL level is generally considered a protective factor against cardiovascular disease, including hypertension.
B. A diet high in potassium: A diet high in potassium is often associated with a lower risk of hypertension. Potassium helps balance sodium levels and supports healthy blood pressure.
C. Obstructive sleep apnea (OSA): This is the correct answer. Obstructive sleep apnea is a known risk factor for hypertension. The repeated episodes of interrupted breathing during sleep can contribute to increased blood pressure.
D. Taking benazepril: Benazepril is an angiotensin-converting enzyme (ACE) inhibitor commonly used to treat hypertension. While it is used to manage high blood pressure, taking the medication itself is not a risk factor for developing hypertension.
A nurse is providing discharge instructions for a client who has congestive heart failure. Which of the following client statements indicates to the nurse that the teaching was effective?
A. "I will take my diuretic before sleep and drink fluids during the day.
"I will take my diuretic before sleep and drink fluids during the day": This statement is not correct. Diuretics are usually taken in the morning to avoid disrupting sleep with increased urination at night. Additionally, fluid intake is generally restricted in congestive heart failure to manage fluid balance.
B. I plan to slow down if I am tired the day after exercising."
"I plan to slow down if I am tired the day after exercising": This statement reflects an understanding of the need to manage activity levels and recognize the signs of overexertion, which is crucial for clients with congestive heart failure. Pacing activities and allowing for adequate rest can help prevent exacerbations of heart failure symptoms.
C. "I will read food labels and limit my sodium to 4 grams per day."
"I will read food labels and limit my sodium to 4 grams per day": This is incorrect. Limiting sodium intake is a key component of heart failure management. The recommended sodium intake for individuals with heart failure is often much lower than 4 grams per day, typically around 2 grams or less.
D. "I should use naproxen to manage discomfort."
"I should use naproxen to manage discomfort": Using nonsteroidal anti-inflammatory drugs (NSAIDs) like naproxen can contribute to fluid retention and worsen heart failure symptoms. This statement is not indicative of effective teaching.
Full Explanation
Correct answer: B
A. "I will take my diuretic before sleep and drink fluids during the day": This statement is not correct. Diuretics are usually taken in the morning to avoid disrupting sleep with increased urination at night. Additionally, fluid intake is generally restricted in congestive heart failure to manage fluid balance.
B. "I plan to slow down if I am tired the day after exercising": This statement reflects an understanding of the need to manage activity levels and recognize the signs of overexertion, which is crucial for clients with congestive heart failure. Pacing activities and allowing for adequate rest can help prevent exacerbations of heart failure symptoms.
C. "I will read food labels and limit my sodium to 4 grams per day": This is incorrect. Limiting sodium intake is a key component of heart failure management. The recommended sodium intake for individuals with heart failure is often much lower than 4 grams per day, typically around 2 grams or less.
D. "I should use naproxen to manage discomfort": Using nonsteroidal anti-inflammatory drugs (NSAIDs) like naproxen can contribute to fluid retention and worsen heart failure symptoms. This statement is not indicative of effective teaching.
A home health nurse visits a client who has COPD and receives oxygen at 2 L/min via nasal cannula. The client reports difficulty breathing. Which of the following actions is the nurse's priority?
A. Call emergency services for the client.
Call emergency services for the client: While difficulty breathing is a concerning symptom, the immediate priority is to assess the client's respiratory status to determine the cause and appropriate interventions. Calling emergency services may be necessary based on the assessment findings, but assessment comes first.
B. Increase the oxygen flow to 3 L/min.
Increase the oxygen flow to 3 L/min: Adjusting oxygen flow may be part of the intervention, but it should be based on a comprehensive assessment of the client's respiratory status. Simply increasing the oxygen flow without a thorough assessment may not address the underlying issue.
C. Have the client cough and expectorate secretions.
Have the client cough and expectorate secretions: This action may be appropriate if the client is experiencing difficulty breathing due to increased bronchial secretions. However, assessment is needed to determine the cause of the difficulty breathing before implementing interventions.
D. Assess the client's respiratory status.
Assess the client's respiratory status: This is the correct answer. Assessment is the priority when a client with COPD on oxygen reports difficulty breathing. The nurse should gather information about the client's respiratory rate, effort, oxygen saturation, lung sounds, and overall respiratory distress to determine the appropriate course of action.
Full Explanation
A. Call emergency services for the client: While difficulty breathing is a concerning symptom, the immediate priority is to assess the client's respiratory status to determine the cause and appropriate interventions. Calling emergency services may be necessary based on the assessment findings, but assessment comes first.
B. Increase the oxygen flow to 3 L/min: Adjusting oxygen flow may be part of the intervention, but it should be based on a comprehensive assessment of the client's respiratory status. Simply increasing the oxygen flow without a thorough assessment may not address the underlying issue.
C. Have the client cough and expectorate secretions: This action may be appropriate if the client is experiencing difficulty breathing due to increased bronchial secretions. However, assessment is needed to determine the cause of the difficulty breathing before implementing interventions.
D. Assess the client's respiratory status: This is the correct answer. Assessment is the priority when a client with COPD on oxygen reports difficulty breathing. The nurse should gather information about the client's respiratory rate, effort, oxygen saturation, lung sounds, and overall respiratory distress to determine the appropriate course of action.