Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is reviewing the plan of care for a group of clients. The nurse should identify that informed consent is required for which of the following procedures?
A. Irrigation of a wound with antibiotic solution
Wound irrigation with an antibiotic solution is a standard nursing intervention for wound care and does not usually involve invasive procedures. Informed consent is not typically required for this procedure.
B. Administration of an iron injection using Z-track technique
The administration of an iron injection using the Z-track technique is a standard nursing procedure. While it involves an injection, it is not typically considered an invasive procedure that would require informed consent.
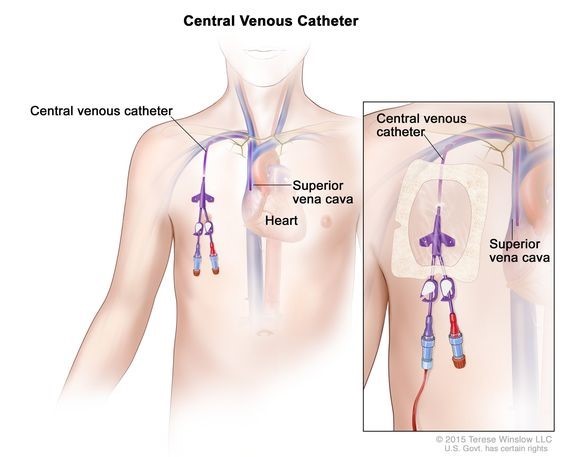
C. Placement of a central venous catheter
Informed consent is a legal and ethical requirement for certain medical procedures. It involves providing the client with clear and comprehensive information about the procedure, including its risks, benefits, alternatives, and expected outcomes. The client must understand the information provided and voluntarily give their consent before the procedure can be performed. Placement of a central venous catheter is an invasive procedure that carries risks and potential complications, making it necessary to obtain informed consent from the client.
D. Insertion of a nasogastric tube
Insertion of a nasogastric tube is a common procedure that involves passing a tube through the nose and into the stomach for various purposes, such as feeding, decompression, or medication administration. While it is an invasive procedure, it is often performed in emergency or critical care situations where the client's immediate well-being takes precedence. Informed consent may not be feasible or necessary in these situations, depending on the context and urgency.
This question is an excerpt from Nurse Dive's nursing test bank - ATI PN Comprehensive Predictor 2023 - Proctored Exam 1. Take the full exam now
Full Explanation
Informed consent is a legal and ethical requirement for certain medical procedures. It involves providing the client with clear and comprehensive information about the procedure, including its risks, benefits, alternatives, and expected outcomes. The client must understand the information provided and voluntarily give their consent before the procedure can be performed.
Placement of a central venous catheter is an invasive procedure that carries risks and potential complications, making it necessary to obtain informed consent from the client.
Wound irrigation with an antibiotic solution is a standard nursing intervention for wound care and does not usually involve invasive procedures. Informed consent is not typically required for this procedure.
The administration of an iron injection using the Z-track technique is a standard nursing procedure. While it involves an injection, it is not typically considered an invasive procedure that would require informed consent.
Insertion of a nasogastric tube is a common procedure that involves passing a tube through the nose and into the stomach for various purposes, such as feeding, decompression, or medication administration. While it is an invasive procedure, it is often performed in emergency or critical care situations where the client's immediate well-being takes precedence. Informed consent may not be feasible or necessary in these situations, depending on the context and urgency.
Similar Questions
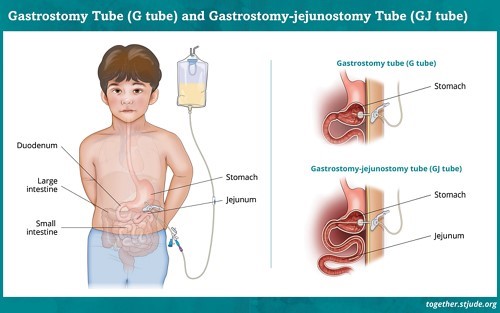
A nurse is providing site care for a child who has a gastrostomy enteral tube. Which of the following actions should the nurse take?
A. Secure the tubing to the child's abdomen.
Securing the tubing to the child's abdomen helps prevent accidental dislodgement or pulling of the gastrostomy tube. This can be done using appropriate securing devices, such as adhesive dressings or commercially available tube holders, as recommended by the healthcare provider.
B. Attach an extension tube to the site's opening prior to use.
Some gastrostomy tubes require an extension set for feeding, especially low-profile devices (e.g., button-type gastrostomy tubes). This extension makes it easier to administer feeds or medications and can be removed afterward. However, this is not typically part of routine site care.
C. Apply water-soluble lubricant to the site.
Applying lubricant to the site is not necessary or recommended. The gastrostomy tube should be kept clean and dry. If any secretions or debris are present, they should be gently cleaned with mild soap and water, followed by thorough rinsing and drying.
D. Tape the tube to the child's cheek.
Taping the tube to the child's cheek is not a recommended practice. It can cause skin irritation, discomfort, or even accidental removal of the tube. Proper securing of the tube to the abdomen using appropriate devices is the preferred method to prevent dislodgement.
Full Explanation
A. Securing the tubing to the child's abdomen helps prevent accidental dislodgement or pulling of the gastrostomy tube. This can be done using appropriate securing devices, such as adhesive dressings or commercially available tube holders, as recommended by the healthcare provider.
B. Some gastrostomy tubes require an extension set for feeding, especially low-profile devices (e.g., button-type gastrostomy tubes). This extension makes it easier to administer feeds or medications and can be removed afterward. However, this is not typically part of routine site care.
C. Applying lubricant to the site is not necessary or recommended. The gastrostomy tube should be kept clean and dry. If any secretions or debris are present, they should be gently cleaned with mild soap and water, followed by thorough rinsing and drying.
D. Taping the tube to the child's cheek is not a recommended practice. It can cause skin irritation, discomfort, or even accidental removal of the tube. Proper securing of the tube to the abdomen using appropriate devices is the preferred method to prevent dislodgement.
A nurse is contributing to an in-service for newly licensed nurses about situations requiring an incident report. Which of the following examples should the nurse include?
A. A nurse discovers that an electronic IV pump delivered twice the prescribed amount of fluid to a client.
An incident report is a tool used to document any unexpected or adverse event that occurs in the healthcare setting. It is important to report incidents to ensure proper investigation, analysis, and implementation of measures to prevent future occurrences. In this example, the incident involves an error with an electronic IV pump resulting in the delivery of an incorrect amount of fluid, which can have serious implications for the client's safety and well-being.
B. A nurse discovers that a client's family member has administered a PCA dose.
While it is concerning that a client's family member administered a patient-controlled analgesia (PCA) dose, it is more appropriate to address this situation through immediate intervention, education, and communication with the healthcare provider. An incident report may not be necessary unless there are further complications or system issues related to this incident.
C. A nurse observes another nurse remove wrist restraints one at a time from a client who is currently calm.
While the observation of improper restraint removal raises concerns about proper restraint protocol, it is more appropriate to address this situation through immediate intervention and communication with the involved nurse and healthcare provider. Depending on the severity of the situation, an incident report may or may not be warranted, but it is not the primary action in this case.
D. A nurse observes a client vomiting after receiving an oral pain medication.
While it is important to assess and address the client's condition and any adverse reactions, such as vomiting after receiving medication, it may not necessarily require an incident report. The nurse should assess the client, notify the healthcare provider, and document the incident appropriately in the client's medical record.
Full Explanation
An incident report is a tool used to document any unexpected or adverse event that occurs in the healthcare setting. It is important to report incidents to ensure proper investigation, analysis, and implementation of measures to prevent future occurrences.
In this example, the incident involves an error with an electronic IV pump resulting in the delivery of an incorrect amount of fluid, which can have serious implications for the client's safety and well-being.
The other examples listed may require further actions but may not necessarily require an incident report:
- A nurse discovers that a client's family member has administered a PCA dose: While it is concerning that a client's family member administered a patient-controlled analgesia (PCA) dose, it is more appropriate to address this situation through immediate intervention, education, and communication with the healthcare provider. An incident report may not be necessary unless there are further complications or system issues related to this incident.
- A nurse observes another nurse remove wrist restraints one at a time from a client who is currently calm: While the observation of improper restraint removal raises concerns about proper restraint protocol, it is more appropriate to address this situation through immediate intervention and communication with the involved nurse and healthcare provider. Depending on the severity of the situation, an incident report may or may not be warranted, but it is not the primary action in this case.
- A nurse observes a client vomiting after receiving an oral pain medication: While it is important to assess and address the client's condition and any adverse reactions, such as vomiting after receiving medication, it may not necessarily require an incident report. The nurse should assess the client, notify the healthcare provider, and document the incident appropriately in the client's medical record.
A nurse is reinforcing teaching about laboratory testing with a client.
Which of the following findings should the nurse include as an indicator of infection?
A. Increased erythrocyte sedimentation rate
Increased erythrocyte sedimentation rate (ESR) is a non-specific marker of inflammation in the body. In the presence of an infection, the ESR tends to rise due to increased levels of acute-phase reactants, such as fibrinogen and globulins. However, it is important to note that an increased ESR alone does not diagnose a specific infection but rather indicates the presence of inflammation or infection.
B. Decreased platelets
Should not be included because they are not typically associated with infection. Low platelet levels (thrombocytopenia) may occur due to various reasons, such as certain medications, immune disorders, or bone marrow problems, but they are not directly linked to infections.
C. Increased iron level
Should not be included because it is not a typical finding in an active infection. In fact, during an infection, iron levels tend to decrease in response to the body's efforts to withhold iron from pathogens, as most microorganisms require iron for their growth and survival.
D. Decreased hemoglobin
Should not be included because it is not directly indicative of an infection. A decrease in hemoglobin levels may be associated with conditions such as anaemia, blood loss, or certain chronic diseases, but it is not a specific marker for infection.
Full Explanation
Explanation
A. Increased erythrocyte sedimentation rate
A. Increased erythrocyte sedimentation rate (ESR) is a non-specific marker of inflammation in the body. In the presence of an infection, the ESR tends to rise due to increased levels of acute-phase reactants, such as fibrinogen and globulins. However, it is important to note that an increased ESR alone does not diagnose a specific infection but rather indicates the presence of inflammation or infection.
Decreased platelets in (option B) should not be included because they are not typically associated with infection. Low platelet levels (thrombocytopenia) may occur due to various reasons, such as certain medications, immune disorders, or bone marrow problems, but they are not directly linked to infections.
Increased iron level in (option C) should not be included because it is not a typical finding in an active infection. In fact, during an infection, iron levels tend to decrease in response to the body's efforts to withhold iron from pathogens, as most microorganisms require iron for their growth and survival.
Decreased haemoglobin in (option D) should not be included because it is not directly indicative of an infection. A decrease in hemoglobin levels may be associated with conditions such as anaemia, blood loss, or certain chronic diseases, but it is not a specific marker for infection.