Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is teaching a community education course about the physical complications related to substance use disorder. Which of the following findings should the nurse include in the discussion as a health risk of heroin use?
A. Nasal septum perforation
A- Nasal septum perforation is commonly associated with the use of cocaine, not heroin.
B. Slowed breathing
Heroin is an opioid drug that depresses the central nervous system, which can lead to respiratory depression. This means that heroin can slow down a person's breathing rate, potentially leading to shallow breathing or even stopping of breathing altogether. This is a life-threatening complication and one of the most significant dangers of heroin use.
C. Acute pancreatitis
C- Acute pancreatitis is not a commonly reported complication of heroin use.
D. Permanent short-term memory loss
D- Permanent short-term memory loss is not a specific complication of heroin use, though chronic substance abuse can lead to cognitive impairments and memory problems in general.
This question is an excerpt from Nurse Dive's nursing test bank - Fall 2022 N 517 Mental Health Proctored Exam 2. Take the full exam now
Full Explanation
Heroin is an opioid drug that depresses the central nervous system, which can lead to respiratory depression. This means that heroin can slow down a person's breathing rate, potentially leading to shallow breathing or even stopping of breathing altogether. This is a life-threatening complication and one of the most significant dangers of heroin use.
The other options listed are associated with other substances or conditions:
A- Nasal septum perforation is commonly associated with the use of cocaine, not heroin.
C- Acute pancreatitis is not a commonly reported complication of heroin use.
D- Permanent short-term memory loss is not a specific complication of heroin use, though chronic substance abuse can lead to cognitive impairments and memory problems in general.

Similar Questions
A nurse is caring for an adolescent female who has an eating disorder. The client is 162.6 cm (64 in) tall and weighs 38.56 kg (85 lb). Upon assessment, which of the following manifestations should the nurse expect? (Select all that apply.)
A. Amenorrhea
A- Amenorrhea: Amenorrhea refers to the absence of menstruation, which is commonly seen in individuals with eating disorders, particularly in cases of severe weight loss or malnutrition.
B. Altered body image
B- Altered body image: Individuals with eating disorders often have a distorted perception of their body shape and size. They may see themselves as overweight or have a negative body image, even when they are significantly underweight.
C. Hyperactivity
C- Hyperactivity: Some individuals with eating disorders may exhibit excessive physical activity or restlessness. This hyperactivity can be a result of increased energy expenditure, driven by a fear of weight gain or a compulsive need to burn calories.
D. Verbalized desire to gain weight
D- Verbalized desire to gain weight is not typically expected in individuals with eating disorders. They may express a desire to lose weight or have a fear of gaining weight instead.
E. Bradycardia
E- Bradycardia: Bradycardia, or a slow heart rate, is a common finding in individuals with severe malnutrition or very low body weight. It can be a result of the body's adaptive response to conserve energy in a state of limited food intake.
Full Explanation
When caring for an adolescent female with an eating disorder, the nurse should expect the following manifestations:
A- Amenorrhea: Amenorrhea refers to the absence of menstruation, which is commonly seen in individuals with eating disorders, particularly in cases of severe weight loss or malnutrition.
B- Altered body image: Individuals with eating disorders often have a distorted perception of their body shape and size. They may see themselves as overweight or have a negative body image, even when they are significantly underweight.
C- Hyperactivity: Some individuals with eating disorders may exhibit excessive physical activity or restlessness. This hyperactivity can be a result of increased energy expenditure, driven by a fear of weight gain or a compulsive need to burn calories.
E- Bradycardia: Bradycardia, or a slow heart rate, is a common finding in individuals with severe malnutrition or very low body weight. It can be a result of the body's adaptive response to conserve energy in a state of limited food intake.
Incorrect:
D- Verbalized desire to gain weight is not typically expected in individuals with eating disorders. They may express a desire to lose weight or have a fear of gaining weight instead.
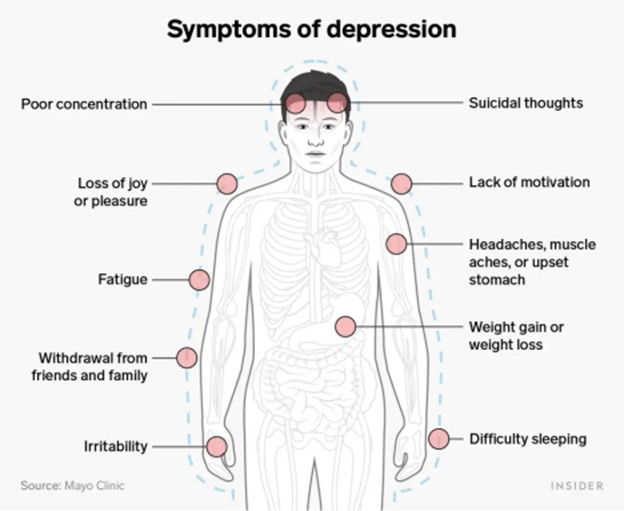
A nurse is caring for an adolescent who is experiencing indications of depression. Which of the following findings should the nurse expect? all that apply.)
A. Irritability
A- Irritability: Depression can manifest as increased irritability or anger, especially in adolescents. They may become easily annoyed or frustrated.
B. Insomnia
B- Insomnia: Sleep disturbances are common in depression. Adolescents may experience difficulty falling asleep, staying asleep, or have restless and disturbed sleep.
C. Chronic pain
C- Chronic pain: Depression can be associated with physical symptoms, including chronic pain. Adolescents may complain of headaches, stomachaches, or other unexplained physical discomfort.
D. Low self-esteem
D- Low self-esteem: Depression often involves feelings of worthlessness, guilt, and low self-esteem. Adolescents may have negative thoughts about themselves, feel inadequate, or have a distorted self-perception.
E. Euphoria
E- Euphoria, on the other hand, is not a typical finding in depression. It refers to an intense state of happiness or excitement, which is not consistent with the overall mood of depression.
Full Explanation
When caring for an adolescent experiencing indications of depression, the nurse should expect the following findings:
A- Irritability: Depression can manifest as increased irritability or anger, especially in adolescents. They may become easily annoyed or frustrated.
B- Insomnia: Sleep disturbances are common in depression. Adolescents may experience difficulty falling asleep, staying asleep, or have restless and disturbed sleep.
C- Chronic pain: Depression can be associated with physical symptoms, including chronic pain. Adolescents may complain of headaches, stomachaches, or other unexplained physical discomfort.
D- Low self-esteem: Depression often involves feelings of worthlessness, guilt, and low self-esteem. Adolescents may have negative thoughts about themselves, feel inadequate, or have a distorted self-perception.
Incorrect:
E- Euphoria, on the other hand, is not a typical finding in depression. It refers to an intense state of happiness or excitement, which is not consistent with the overall mood of depression.
A nurse is caring for a client who reports acute, moderate anxiety. Which of the following is the priority nursing action?
A. Instruct the client to remember past coping mechanisms.
While the other options are also beneficial interventions for managing anxiety, they are not the priority in this situation. Instructing the client to remember past coping mechanisms (Option A) can be helpful, but the immediate presence of the nurse is more important to provide immediate support.
B. Provide a diverting activity.
Providing a diverting activity (Option B) can be beneficial to distract the client from their anxiety, but it does not address the underlying anxiety or provide direct support.
C. Encourage verbalization of feelings.
Encouraging verbalization of feelings (Option C) is important for therapeutic communication, but it may not be the initial priority when the client is experiencing acute anxiety.
D. Remain with the client.
By remaining with the client, the nurse provides a sense of support and security. This presence can help alleviate the client's anxiety and provide reassurance. It also ensures that the nurse is available to assess the client's condition, offer therapeutic communication, and intervene if the anxiety escalates or the client becomes overwhelmed.
Full Explanation
By remaining with the client, the nurse provides a sense of support and security. This presence can help alleviate the client's anxiety and provide reassurance. It also ensures that the nurse is available to assess the client's condition, offer therapeutic communication, and intervene if the anxiety escalates or the client becomes overwhelmed.
While the other options are also beneficial interventions for managing anxiety, they are not the priority in this situation. Instructing the client to remember past coping mechanisms (Option A) can be helpful, but the immediate presence of the nurse is more important to provide immediate support.
Providing a diverting activity (Option B) can be beneficial to distract the client from their anxiety, but it does not address the underlying anxiety or provide direct support.
Encouraging verbalization of feelings (Option C) is important for therapeutic communication, but it may not be the initial priority when the client is experiencing acute anxiety.