Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse is teaching a group of clients about risk factors for developing diabetes mellitus. The nurse should include which of the following as a risk factor for diabetes?
A. Abdominal obesity
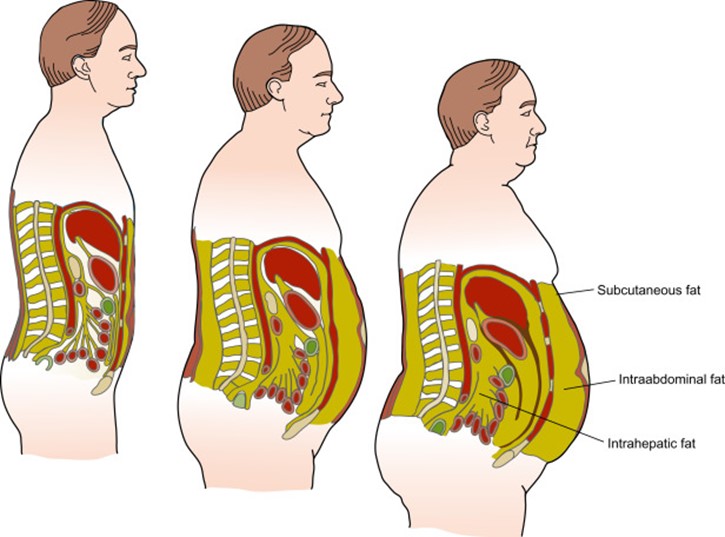
Abdominal obesity is a risk factor for developing diabetes mellitus. Abdominal obesity, also known as central obesity or visceral fat, is the accumulation of fat around the abdomen and organs. Abdominal obesity can cause insulin resistance, inflammation, and metabolic syndrome, which are all associated with diabetes.
B. Elevated HDL level
Elevated HDL level is not a risk factor for developing diabetes mellitus. HDL stands for high-density lipoprotein, which is a type of cholesterol that carries excess cholesterol from the tissues to the liver for disposal. HDL is also known as "good" cholesterol, as it helps protect against heart disease and stroke. A high HDL level is desirable and beneficial for health.
C. History of hypotension
History of hypotension is not a risk factor for developing diabetes mellitus. Hypotension means low blood pressure, which is usually defined as less than 90/60 mm Hg. Hypotension can cause symptoms such as dizziness, fainting, fatigue, and blurred vision. Hypotension can be caused by dehydration, blood loss, medication side effects, or other conditions.
D. History of hyperthyroidism
History of hyperthyroidism is not a risk factor for developing diabetes mellitus. Hyperthyroidism means overactive thyroid gland, which produces too much thyroid hormone. Thyroid hormone regulates metabolism, growth, and development. Hyperthyroidism can cause symptoms such as weight loss, nervousness, palpitations, heat intolerance, and insomnia. Hyperthyroidism can be caused by Graves' disease, thyroid nodules, or thyroiditis.
This question is an excerpt from Nurse Dive's nursing test bank - RN Nutrition 2019 Nexy Updated 2023 Proctored Exam. Take the full exam now
Full Explanation
Choice A reason: Abdominal obesity is a risk factor for developing diabetes mellitus. Abdominal obesity, also known as central obesity or visceral fat, is the accumulation of fat around the abdomen and organs. Abdominal obesity can cause insulin resistance, inflammation, and metabolic syndrome, which are all associated with diabetes.
Choice B reason: Elevated HDL level is not a risk factor for developing diabetes mellitus. HDL stands for high-density lipoprotein, which is a type of cholesterol that carries excess cholesterol from the tissues to the liver for disposal. HDL is also known as "good" cholesterol, as it helps protect against heart disease and stroke. A high HDL level is desirable and beneficial for health.
Choice C reason: History of hypotension is not a risk factor for developing diabetes mellitus. Hypotension means low blood pressure, which is usually defined as less than 90/60 mm Hg. Hypotension can cause symptoms such as dizziness, fainting, fatigue, and blurred vision. Hypotension can be caused by dehydration, blood loss, medication side effects, or other conditions.
Choice D reason: History of hyperthyroidism is not a risk factor for developing diabetes mellitus. Hyperthyroidism means overactive thyroid gland, which produces too much thyroid hormone. Thyroid hormone regulates metabolism, growth, and development. Hyperthyroidism can cause symptoms such as weight loss, nervousness, palpitations, heat intolerance, and insomnia. Hyperthyroidism can be caused by Graves' disease, thyroid nodules, or thyroiditis.
Similar Questions
A nurse is reviewing the laboratory findings of a client who has heart failure. Which of the following findings indicates that the client is experiencing fluid volume excess?
A. Creatinine 0.8 mg/dL
Creatinine 0.8 mg/dL is within the normal range (0.6-1.2), and it does not indicate fluid volume excess. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys. High creatinine levels can indicate kidney damage or impaired renal function.
B. Hgb 15 g/dL
Hgb 15 g/dL is within the normal range (13-17 for men, 12-16 for women), and it does not indicate fluid volume excess. Hgb stands for hemoglobin, which is a protein in red blood cells that carries oxygen to the tissues. Low hemoglobin levels can indicate anemia, bleeding, or hemolysis.
C. BUN 18 mg/dL
BUN 18 mg/dL is within the normal range (7-20), and it does not indicate fluid volume excess. BUN stands for blood urea nitrogen, which is a waste product of protein metabolism that is filtered by the kidneys. High BUN levels can indicate dehydration, kidney damage, or high protein intake.
D. Sodium 149 mEq/L
Sodium 149 mEq/L is high and indicates fluid volume excess. Sodium is an electrolyte that helps maintain fluid balance, blood pressure, and nerve impulses. High sodium levels can cause fluid retention, edema, hypertension, and heart failure.
Full Explanation
Choice A reason: Creatinine 0.8 mg/dL is within the normal range (0.6-1.2), and it does not indicate fluid volume excess. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys. High creatinine levels can indicate kidney damage or impaired renal function.
Choice B reason: Hgb 15 g/dL is within the normal range (13-17 for men, 12-16 for women), and it does not indicate fluid volume excess. Hgb stands for hemoglobin, which is a protein in red blood cells that carries oxygen to the tissues. Low hemoglobin levels can indicate anemia, bleeding, or hemolysis.
Choice C reason: BUN 18 mg/dL is within the normal range (7-20), and it does not indicate fluid volume excess. BUN stands for blood urea nitrogen, which is a waste product of protein metabolism that is filtered by the kidneys. High BUN levels can indicate dehydration, kidney damage, or high protein intake.
Choice D reason: Sodium 149 mEq/L is high and indicates fluid volume excess. Sodium is an electrolyte that helps maintain fluid balance, blood pressure, and nerve impulses. High sodium levels can cause fluid retention, edema, hypertension, and heart failure.
A nurse is teaching an older adult client about vitamin D deficiency. The nurse should encourage the client to consume an adequate amount of vitamin D to prevent which of the following complications?
A. Dry eyes
Dry eyes are not caused by vitamin D deficiency, but by other factors such as aging, medication, environmental conditions, or eye diseases. Vitamin D does not have a direct role in eye health or function.
B. Fractures
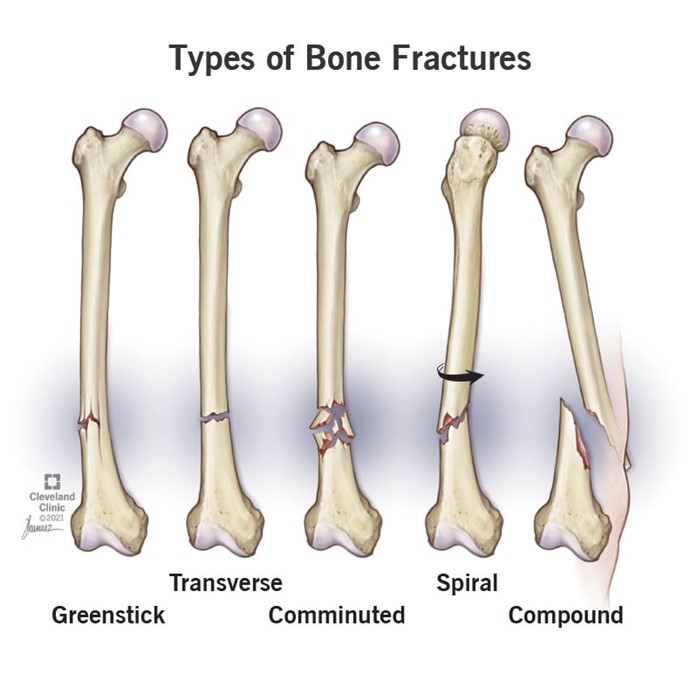
Fractures are caused by vitamin D deficiency, as vitamin D helps the body absorb calcium, which is essential for bone health and strength. Vitamin D deficiency can lead to osteoporosis, a condition in which the bones become brittle and prone to breaking.
C. Infection
Infection is not caused by vitamin D deficiency, but by other factors such as exposure to pathogens, weakened immune system, or poor hygiene. Vitamin D may have some role in modulating immune responses, but it is not a primary factor in preventing infection.
D. Swelling
Swelling is not caused by vitamin D deficiency, but by other factors such as injury, inflammation, fluid retention, or allergic reaction. Vitamin D does not have a direct role in regulating fluid balance or reducing inflammation.
Full Explanation
Choice A reason: Dry eyes are not caused by vitamin D deficiency, but by other factors such as aging, medication, environmental conditions, or eye diseases. Vitamin D does not have a direct role in eye health or function.
Choice B reason: Fractures are caused by vitamin D deficiency, as vitamin D helps the body absorb calcium, which is essential for bone health and strength. Vitamin D deficiency can lead to osteoporosis, a condition in which the bones become brittle and prone to breaking.
Choice C reason: Infection is not caused by vitamin D deficiency, but by other factors such as exposure to pathogens, weakened immune system, or poor hygiene. Vitamin D may have some role in modulating immune responses, but it is not a primary factor in preventing infection.
Choice D reason: Swelling is not caused by vitamin D deficiency, but by other factors such as injury, inflammation, fluid retention, or allergic reaction. Vitamin D does not have a direct role in regulating fluid balance or reducing inflammation.
A nurse is providing dietary teaching to a client newly diagnosed with celiac disease. Which of the following information should the nurse include in the teaching?
A. Dietary restrictions will eventually allow the intake of gluten to resume.
Dietary restrictions will not eventually allow the intake of gluten to resume. Gluten is a protein found in wheat, barley, rye, and some oats. It causes damage to the small intestine in people with celiac disease. The only treatment for celiac disease is a lifelong gluten-free diet.
B. This condition may cause secondary lactose intolerance.
This condition may cause secondary lactose intolerance. Lactose is a sugar found in milk and dairy products. It is broken down by an enzyme called lactase in the small intestine. People with celiac disease may have reduced levels of lactase due to the damage to the small intestine caused by gluten. This can lead to lactose intolerance, which is the inability to digest lactose properly. Symptoms of lactose intolerance include bloating, gas, diarrhea, and abdominal pain after consuming dairy products.
C. Nutritional therapy for this condition includes limiting proteins and calories.
Nutritional therapy for this condition does not include limiting proteins and calories. People with celiac disease need adequate amounts of proteins and calories to maintain their health and prevent malnutrition. They also need to ensure that they get enough vitamins, minerals, and fiber from gluten-free sources.
D. A normal diet can resume after a period of remission.
A normal diet cannot resume after a period of remission. Celiac disease is a chronic autoimmune disorder that does not have a cure. Even if the symptoms improve or disappear, the damage to the small intestine can still occur if gluten is consumed. Therefore, a strict gluten-free diet must be followed for life.
Full Explanation
Choice A reason: Dietary restrictions will not eventually allow the intake of gluten to resume. Gluten is a protein found in wheat, barley, rye, and some oats. It causes damage to the small intestine in people with celiac disease. The only treatment for celiac disease is a lifelong gluten-free diet.
Choice B reason: This condition may cause secondary lactose intolerance. Lactose is a sugar found in milk and dairy products. It is broken down by an enzyme called lactase in the small intestine. People with celiac disease may have reduced levels of lactase due to the damage to the small intestine caused by gluten. This can lead to lactose intolerance, which is the inability to digest lactose properly. Symptoms of lactose intolerance include bloating, gas, diarrhea, and abdominal pain after consuming dairy products.
Choice C reason: Nutritional therapy for this condition does not include limiting proteins and calories. People with celiac disease need adequate amounts of proteins and calories to maintain their health and prevent malnutrition. They also need to ensure that they get enough vitamins, minerals, and fiber from gluten-free sources.
Choice D reason: A normal diet cannot resume after a period of remission. Celiac disease is a chronic autoimmune disorder that does not have a cure. Even if the symptoms improve or disappear, the damage to the small intestine can still occur if gluten is consumed. Therefore, a strict gluten-free diet must be followed for life.