Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
A nurse suspects a client has diabetes insipidus. What are the priority interventions? Select all that apply.
A. Monitor for hypernatremia.
Hypernatremia, or high sodium levels in the blood, is a common complication of diabetes insipidus due to excessive water loss and insufficient water intake. Monitoring for hypernatremia involves regular blood tests to check sodium levels. Symptoms of hypernatremia include extreme thirst, confusion, muscle twitching, and seizures. Early detection and management are crucial to prevent severe complications.
B. Monitor neuro status.
Monitoring neurological status is essential in patients with diabetes insipidus because severe hypernatremia can lead to neurological symptoms such as confusion, irritability, seizures, and even coma. Regular assessments of mental status, level of consciousness, and neurological function help in early detection of complications and timely intervention.
C. Monitor for hyponatremia.
While hyponatremia (low sodium levels) is less common in diabetes insipidus, it can occur if there is excessive water intake without adequate sodium replacement. Symptoms include headache, nausea, vomiting, confusion, and seizures. Monitoring sodium levels helps in maintaining a balance and preventing complications.
D. Monitor urine specific gravity.
Urine specific gravity measures the concentration of solutes in the urine. In diabetes insipidus, urine is typically very dilute, with a specific gravity of less than 1.005. Regular monitoring helps in assessing the effectiveness of treatment and the patient’s hydration status. It also aids in differentiating diabetes insipidus from other conditions with similar symptoms.
E. Monitor strict I&O.
Strict monitoring of intake and output (I&O) is crucial in managing diabetes insipidus. This involves accurately measuring all fluids consumed and excreted to ensure proper hydration and electrolyte balance. It helps in identifying trends in fluid loss and guiding appropriate fluid replacement therapy.
This question is an excerpt from Nurse Dive's nursing test bank - Final Med Surg Comprehensive Proctored Exam (Brooklyn University). Take the full exam now
Full Explanation
Choice A: Monitor for hypernatremia.
Hypernatremia, or high sodium levels in the blood, is a common complication of diabetes insipidus due to excessive water loss and insufficient water intake. Monitoring for hypernatremia involves regular blood tests to check sodium levels. Symptoms of hypernatremia include extreme thirst, confusion, muscle twitching, and seizures. Early detection and management are crucial to prevent severe complications.
Choice B: Monitor neuro status.
Monitoring neurological status is essential in patients with diabetes insipidus because severe hypernatremia can lead to neurological symptoms such as confusion, irritability, seizures, and even coma. Regular assessments of mental status, level of consciousness, and neurological function help in early detection of complications and timely intervention.
Choice C: Monitor for hyponatremia.
While hyponatremia (low sodium levels) is less common in diabetes insipidus, it can occur if there is excessive water intake without adequate sodium replacement. Symptoms include headache, nausea, vomiting, confusion, and seizures. Monitoring sodium levels helps in maintaining a balance and preventing complications.
Choice D: Monitor urine specific gravity.
Urine specific gravity measures the concentration of solutes in the urine. In diabetes insipidus, urine is typically very dilute, with a specific gravity of less than 1.005. Regular monitoring helps in assessing the effectiveness of treatment and the patient’s hydration status. It also aids in differentiating diabetes insipidus from other conditions with similar symptoms.
Choice E: Monitor strict I&O.
Strict monitoring of intake and output (I&O) is crucial in managing diabetes insipidus. This involves accurately measuring all fluids consumed and excreted to ensure proper hydration and electrolyte balance. It helps in identifying trends in fluid loss and guiding appropriate fluid replacement therapy.
Similar Questions
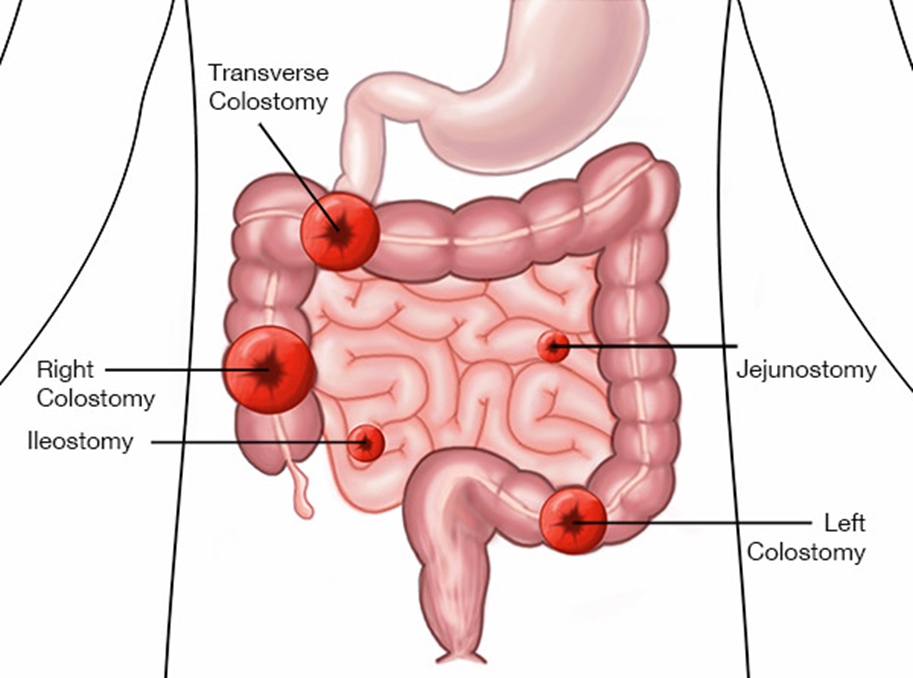
The nurse is caring for a client with an ileostomy because of inflammatory bowel disease. Which assessment findings indicate to the nurse that the ileostomy is functioning as expected? Select all that apply.
A. Formed stool in collection pouch.
Formed stool in the collection pouch is not expected in an ileostomy. The output from an ileostomy is typically liquid to semi-liquid because the ileum does not absorb as much water as the colon. If formed stool is present, it may indicate a blockage or other issue that needs to be addressed.
B. Stoma is edematous and bleeding.
An edematous and bleeding stoma is not a normal finding and may indicate complications such as infection, trauma, or poor stoma care. The stoma should be moist and pink, but not swollen or bleeding. Persistent bleeding or significant edema should be reported to a healthcare provider immediately.
C. Stoma is pink and shiny.
A pink and shiny stoma is a sign that the ileostomy is functioning well. This indicates good blood flow and healthy tissue. The stoma should always appear moist and pink, similar to the inside of the mouth. Any deviation from this appearance, such as a pale, dark, or dry stoma, should be evaluated by a healthcare professional.
D. Skin excoriation around the stoma.
Skin excoriation around the stoma is not a normal finding and suggests that the skin is being irritated by the stoma output or the ostomy appliance. Proper skin care and fitting of the ostomy appliance are essential to prevent skin breakdown. If excoriation occurs, it should be treated promptly to prevent further complications.
E. Mucus liquid flows from the stoma.
Mucus liquid flowing from the stoma is expected in an ileostomy. The output is typically liquid to semi-liquid and may contain mucus, which is normal for the small intestine. This type of output indicates that the ileostomy is functioning as intended.
Full Explanation
Choice A: Formed stool in collection pouch
Formed stool in the collection pouch is not expected in an ileostomy. The output from an ileostomy is typically liquid to semi-liquid because the ileum does not absorb as much water as the colon. If formed stool is present, it may indicate a blockage or other issue that needs to be addressed.
Choice B: Stoma is edematous and bleeding
An edematous and bleeding stoma is not a normal finding and may indicate complications such as infection, trauma, or poor stoma care. The stoma should be moist and pink, but not swollen or bleeding. Persistent bleeding or significant edema should be reported to a healthcare provider immediately.
Choice C: Stoma is pink and shiny
A pink and shiny stoma is a sign that the ileostomy is functioning well. This indicates good blood flow and healthy tissue. The stoma should always appear moist and pink, similar to the inside of the mouth. Any deviation from this appearance, such as a pale, dark, or dry stoma, should be evaluated by a healthcare professional.
Choice D: Skin excoriation around the stoma
Skin excoriation around the stoma is not a normal finding and suggests that the skin is being irritated by the stoma output or the ostomy appliance. Proper skin care and fitting of the ostomy appliance are essential to prevent skin breakdown. If excoriation occurs, it should be treated promptly to prevent further complications.
Choice E: Mucus liquid flows from the stoma
Mucus liquid flowing from the stoma is expected in an ileostomy. The output is typically liquid to semi-liquid and may contain mucus, which is normal for the small intestine. This type of output indicates that the ileostomy is functioning as intended.
A client experiences impaired swallowing after a stroke and has worked with speech-language pathology on eating. What nursing assessment best indicates that the expected outcome for this problem has been met?
A. Gains 2 lbs (1 kg) after 1 week.
: Gaining weight can be an indicator of improved nutrition, but it does not directly address the client’s ability to swallow safely and effectively. Weight gain could be due to other factors such as fluid retention or changes in metabolism. Therefore, while it is a positive outcome, it is not the best indicator of improved swallowing function.
B. Chooses preferred items from the menu.
: Choosing preferred items from the menu indicates that the client is engaged in their meal planning and has an appetite. However, it does not directly measure the client’s ability to swallow safely. The client might still have difficulty swallowing even if they are choosing their preferred foods.
C. Clearly understands and articulates.
: Clear understanding and articulation are important for communication and can indicate cognitive improvement. However, this choice does not directly relate to the client’s swallowing ability. The primary concern in this scenario is the client’s ability to swallow safely, not their communication skills.
D. Eats 75 to 100% of all meals and snacks.
: Eating 75 to 100% of all meals and snacks is the best indicator that the client has improved their swallowing ability. This choice directly measures the client’s ability to consume food and liquids safely and effectively. It shows that the client can manage their meals without significant difficulty, which is the primary goal of the intervention.
Full Explanation
Choice A Reason:
Gaining weight can be an indicator of improved nutrition, but it does not directly address the client’s ability to swallow safely and effectively. Weight gain could be due to other factors such as fluid retention or changes in metabolism. Therefore, while it is a positive outcome, it is not the best indicator of improved swallowing function.
Choice B Reason:
Choosing preferred items from the menu indicates that the client is engaged in their meal planning and has an appetite. However, it does not directly measure the client’s ability to swallow safely. The client might still have difficulty swallowing even if they are choosing their preferred foods.
Choice C Reason:
Clear understanding and articulation are important for communication and can indicate cognitive improvement. However, this choice does not directly relate to the client’s swallowing ability. The primary concern in this scenario is the client’s ability to swallow safely, not their communication skills.
Choice D Reason:
Eating 75 to 100% of all meals and snacks is the best indicator that the client has improved their swallowing ability. This choice directly measures the client’s ability to consume food and liquids safely and effectively. It shows that the client can manage their meals without significant difficulty, which is the primary goal of the intervention.
The nurse is planning care for a client diagnosed with SIADH. Which of the following would be included in the plan of care? Select all that apply.
A. Administer 0.45% NS at 50 mL/h.
: Administering 0.45% NS (normal saline) at 50 mL/h is not appropriate for a client with SIADH (Syndrome of Inappropriate Antidiuretic Hormone Secretion). This solution is hypotonic and can exacerbate the condition by increasing water retention and worsening hyponatremia. Therefore, this choice is not included in the plan of care.
B. Obtain daily weight.
: Obtaining daily weight is crucial for monitoring fluid balance in clients with SIADH. Daily weights help detect fluid retention or loss, which is essential for managing the condition. Accurate weight measurements can indicate changes in fluid status and guide adjustments in treatment.
C. Maintain seizure precautions.
: Maintaining seizure precautions is vital for clients with SIADH because severe hyponatremia can lead to neurological symptoms, including seizures. Implementing seizure precautions helps ensure the client’s safety and allows for prompt intervention if seizures occur.
D. Administer 3% saline as ordered.
: Administering 3% saline as ordered is appropriate for treating severe hyponatremia in clients with SIADH. Hypertonic saline helps increase serum sodium levels, which is critical for correcting the electrolyte imbalance. This intervention should be closely monitored to avoid rapid changes in sodium levels.
E. Encourage fluid intake.
: Encouraging fluid intake is not appropriate for clients with SIADH. The condition is characterized by excessive water retention, and increasing fluid intake can worsen hyponatremia. Instead, fluid restriction is typically recommended to manage the condition effectively.
Full Explanation
Choice A Reason:
Administering 0.45% NS (normal saline) at 50 mL/h is not appropriate for a client with SIADH (Syndrome of Inappropriate Antidiuretic Hormone Secretion). This solution is hypotonic and can exacerbate the condition by increasing water retention and worsening hyponatremia. Therefore, this choice is not included in the plan of care.
Choice B Reason:
Obtaining daily weight is crucial for monitoring fluid balance in clients with SIADH. Daily weights help detect fluid retention or loss, which is essential for managing the condition. Accurate weight measurements can indicate changes in fluid status and guide adjustments in treatment.
Choice C Reason:
Maintaining seizure precautions is vital for clients with SIADH because severe hyponatremia can lead to neurological symptoms, including seizures. Implementing seizure precautions helps ensure the client’s safety and allows for prompt intervention if seizures occur.
Choice D Reason:
Administering 3% saline as ordered is appropriate for treating severe hyponatremia in clients with SIADH. Hypertonic saline helps increase serum sodium levels, which is critical for correcting the electrolyte imbalance. This intervention should be closely monitored to avoid rapid changes in sodium levels.
Choice E Reason:
Encouraging fluid intake is not appropriate for clients with SIADH. The condition is characterized by excessive water retention, and increasing fluid intake can worsen hyponatremia. Instead, fluid restriction is typically recommended to manage the condition effectively.