Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
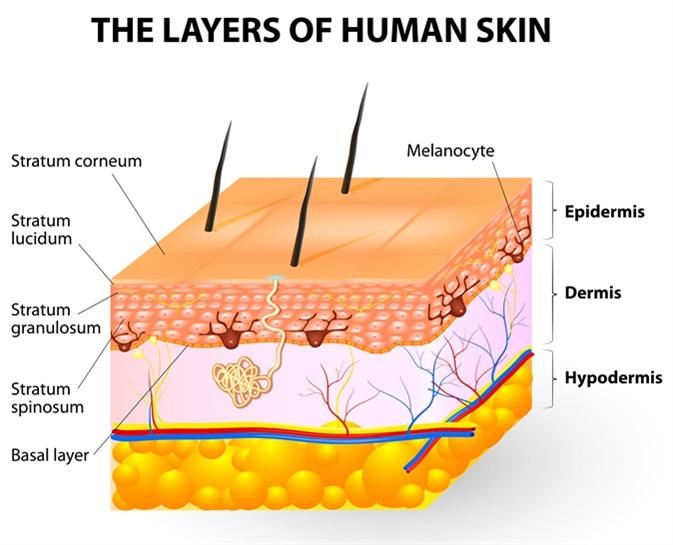
Melanocytes give rise to the pigment melanin, which is responsible for skin color. Where can the melanocytes be found?
A. Loose connective tissue
Loose connective tissue:Melanocytes are not typically found in loose connective tissue. Their primary location is within the epidermis, specifically in the basal layer, where they interact with keratinocytes to produce melanin and contribute to skin color. Loose connective tissue contains collagen and elastin fibers, as well as fibroblasts, but it does not house melanocytes.
B. Epidermis
Epidermis: This is the correct answer. Melanocytes are primarily located in the basal layer of the epidermis, which is the deepest layer of the epidermis. These cells produce melanin, a pigment that helps protect the skin from UV radiation and determines skin color. Melanocytes are interspersed among keratinocytes in the epidermis and transfer melanin to keratinocytes to provide skin pigmentation.
C. Dermis
Dermis:The dermis is the layer of skin beneath the epidermis and consists of connective tissue, blood vessels, nerves, hair follicles, and sweat glands. While the dermis plays a crucial role in supporting and nourishing the epidermis, melanocytes are not primarily located in the dermis. They are confined to the basal layer of the epidermis.
D. Superficial fascia
Superficial fascia:The superficial fascia, also known as the subcutaneous tissue or hypodermis, lies beneath the dermis and consists of adipose (fat) tissue and connective tissue. It provides insulation, energy storage, and cushioning for underlying structures. However, melanocytes are not typically found in the superficial fascia. They are restricted to the epidermis, specifically the basal layer, where they carry out their function of melanin production.
This question is an excerpt from Nurse Dive's nursing test bank - Ati Lpn Med Surg Cohort 6 Proctored Exam. Take the full exam now
Full Explanation
A. Loose connective tissue:
Melanocytes are not typically found in loose connective tissue. Their primary location is within the epidermis, specifically in the basal layer, where they interact with keratinocytes to produce melanin and contribute to skin color. Loose connective tissue contains collagen and elastin fibers, as well as fibroblasts, but it does not house melanocytes.
B. Epidermis:
This is the correct answer. Melanocytes are primarily located in the basal layer of the epidermis, which is the deepest layer of the epidermis. These cells produce melanin, a pigment that helps protect the skin from UV radiation and determines skin color. Melanocytes are interspersed among keratinocytes in the epidermis and transfer melanin to keratinocytes to provide skin pigmentation.
C. Dermis:
The dermis is the layer of skin beneath the epidermis and consists of connective tissue, blood vessels, nerves, hair follicles, and sweat glands. While the dermis plays a crucial role in supporting and nourishing the epidermis, melanocytes are not primarily located in the dermis. They are confined to the basal layer of the epidermis.
D. Superficial fascia:
The superficial fascia, also known as the subcutaneous tissue or hypodermis, lies beneath the dermis and consists of adipose (fat) tissue and connective tissue. It provides insulation, energy storage, and cushioning for underlying structures. However, melanocytes are not typically found in the superficial fascia. They are restricted to the epidermis, specifically the basal layer, where they carry out their function of melanin production.
Similar Questions
A nurse is caring for a client during fluid resuscitation for burns. Which of the following are used to evaluate the success of fluid resuscitation? (Select all that apply.)
A. Blood pressure
Blood pressure:Monitoring blood pressure is a crucial aspect of evaluating fluid resuscitation in burn patients. Adequate fluid resuscitation should help maintain stable blood pressure levels within an acceptable range. Hypotension (low blood pressure) can indicate inadequate fluid resuscitation, leading to poor tissue perfusion and organ function. On the other hand, hypertension (high blood pressure) may suggest fluid overload, which can lead to complications such as pulmonary edema. Therefore, regular monitoring of blood pressure helps assess the effectiveness of fluid resuscitation and guides adjustments in fluid administration rates.
B. Bowel sounds
Bowel sounds:While bowel sounds are important indicators of gastrointestinal motility and function, they are not directly used to evaluate the success of fluid resuscitation in burn patients. Bowel sounds may be assessed for other reasons, such as postoperative recovery or gastrointestinal conditions, but they do not provide specific information about fluid resuscitation status or tissue perfusion.
C. Level of consciousness
Level of consciousness:Assessing the client's level of consciousness is crucial during fluid resuscitation for burns. Changes in consciousness, such as confusion, lethargy, or altered mental status, can indicate inadequate tissue perfusion and oxygenation. A clear and responsive level of consciousness suggests adequate fluid resuscitation and perfusion to vital organs, while alterations in consciousness may prompt further evaluation and adjustment of fluid resuscitation strategies.
D. Urine output
Urine output:Monitoring urine output is a key parameter in evaluating fluid resuscitation in burn patients. Adequate urine output (0.5 to 1 mL/kg/hr in adults) indicates sufficient renal perfusion and function, suggesting effective fluid resuscitation. Decreased urine output or oliguria may indicate inadequate fluid resuscitation, renal impairment, or hypovolemia, requiring reassessment and potential adjustments in fluid administration rates or type of fluids used.
E. Platelet count
Platelet count is an important component of the complete blood count (CBC) and is used to assess clotting function and risk of bleeding. However, platelet count is not specifically used to evaluate the success of fluid resuscitation in burn patients. While clotting parameters may be monitored in burn patients, including platelet count, they are not direct indicators of fluid resuscitation status or tissue perfusion. Other laboratory parameters, such as hemoglobin, hematocrit, electrolyte levels, and arterial blood gases, may be monitored to assess the effectiveness of fluid resuscitation.
Full Explanation
A. Blood pressure:
Monitoring blood pressure is a crucial aspect of evaluating fluid resuscitation in burn patients. Adequate fluid resuscitation should help maintain stable blood pressure levels within an acceptable range. Hypotension (low blood pressure) can indicate inadequate fluid resuscitation, leading to poor tissue perfusion and organ function. On the other hand, hypertension (high blood pressure) may suggest fluid overload, which can lead to complications such as pulmonary edema. Therefore, regular monitoring of blood pressure helps assess the effectiveness of fluid resuscitation and guides adjustments in fluid administration rates.
B. Bowel sounds:
While bowel sounds are important indicators of gastrointestinal motility and function, they are not directly used to evaluate the success of fluid resuscitation in burn patients. Bowel sounds may be assessed for other reasons, such as postoperative recovery or gastrointestinal conditions, but they do not provide specific information about fluid resuscitation status or tissue perfusion.
C. Level of consciousness:
Assessing the client's level of consciousness is crucial during fluid resuscitation for burns. Changes in consciousness, such as confusion, lethargy, or altered mental status, can indicate inadequate tissue perfusion and oxygenation. A clear and responsive level of consciousness suggests adequate fluid resuscitation and perfusion to vital organs, while alterations in consciousness may prompt further evaluation and adjustment of fluid resuscitation strategies.
D. Urine output:
Monitoring urine output is a key parameter in evaluating fluid resuscitation in burn patients. Adequate urine output (0.5 to 1 mL/kg/hr in adults) indicates sufficient renal perfusion and function, suggesting effective fluid resuscitation. Decreased urine output or oliguria may indicate inadequate fluid resuscitation, renal impairment, or hypovolemia, requiring reassessment and potential adjustments in fluid administration rates or type of fluids used.
E. Platelet count:
Platelet count is an important component of the complete blood count (CBC) and is used to assess clotting function and risk of bleeding. However, platelet count is not specifically used to evaluate the success of fluid resuscitation in burn patients. While clotting parameters may be monitored in burn patients, including platelet count, they are not direct indicators of fluid resuscitation status or tissue perfusion. Other laboratory parameters, such as hemoglobin, hematocrit, electrolyte levels, and arterial blood gases, may be monitored to assess the effectiveness of fluid resuscitation.
A nurse is caring for a client with a chronic wound. Which of the following is a systemic cause of chronic wounds?
A. Infection
Infection: While infection can certainly delay wound healing and contribute to the development of chronic wounds, it is more of a local factor rather than a systemic cause. Infections can hinder the normal healing process and lead to tissue damage, inflammation, and prolonged wound healing.
B. Malnutrition
MalnutritionA chronic wound is a wound that fails to progress through the normal stages of healing in an orderly and timely manner. Systemic factors can significantly impact wound healing, and malnutrition is one such systemic cause. Malnutrition, which refers to an inadequate intake or absorption of nutrients essential for healing, can impair the body's ability to repair tissues, fight infection, and generate new cells.
C. Continued pressure
Continued pressure: Prolonged pressure, such as that experienced in pressure ulcers, can lead to tissue ischemia (lack of blood flow) and tissue necrosis, resulting in chronic wounds. However, this is considered a local factor related to the specific site of the wound and pressure-related damage.
D. Venous insufficiency
Venous insufficiency: Venous insufficiency can cause chronic wounds, particularly venous ulcers, due to impaired venous return leading to increased pressure in the veins of the lower extremities. This pressure can result in tissue damage and poor wound healing. While venous insufficiency is a systemic condition, it primarily affects specific areas of the body (such as the lower legs) and is more directly related to the development of localized chronic wounds in those areas.
Full Explanation
A. Infection: While infection can certainly delay wound healing and contribute to the development of chronic wounds, it is more of a local factor rather than a systemic cause. Infections can hinder the normal healing process and lead to tissue damage, inflammation, and prolonged wound healing.
B. Malnutrition
A chronic wound is a wound that fails to progress through the normal stages of healing in an orderly and timely manner. Systemic factors can significantly impact wound healing, and malnutrition is one such systemic cause. Malnutrition, which refers to an inadequate intake or absorption of nutrients essential for healing, can impair the body's ability to repair tissues, fight infection, and generate new cells.
C. Continued pressure: Prolonged pressure, such as that experienced in pressure ulcers, can lead to tissue ischemia (lack of blood flow) and tissue necrosis, resulting in chronic wounds. However, this is considered a local factor related to the specific site of the wound and pressure-related damage.
D. Venous insufficiency: Venous insufficiency can cause chronic wounds, particularly venous ulcers, due to impaired venous return leading to increased pressure in the veins of the lower extremities. This pressure can result in tissue damage and poor wound healing. While venous insufficiency is a systemic condition, it primarily affects specific areas of the body (such as the lower legs) and is more directly related to the development of localized chronic wounds in those areas.
A nurse assesses a patient who is prescribed a medication that inhibits aldosterone secretion and release. For which potential complications will the nurse assess? (Select all that apply.)
A. Serum potassium level of 3.2 mEq/L
A serum potassium level of 3.2 mEq/L indicates hypokalemia, which is a potential complication of inhibiting aldosterone secretion and release. Aldosterone plays a key role in potassium regulation in the body by promoting potassium excretion in the kidneys. When aldosterone secretion is inhibited, potassium excretion decreases, leading to an accumulation of potassium in the bloodstream and resulting in hypokalemia. Symptoms of hypokalemia may include muscle weakness, cramping, irregular heartbeat, and fatigue.
B. Urine output of 1 200 mL in the last 2 hours
Urine output of 1,200 mL in the last 2 hours:This option does not directly relate to complications of inhibiting aldosterone secretion. A urine output of 1,200 mL in the last 2 hours indicates adequate urine production, which is generally a positive sign. However, in the context of inhibiting aldosterone secretion, the nurse would be more concerned about decreased urine output due to potential renal effects.
C. Blood osmolality of 250 mOsm/kg (250 mmol/kg)
Blood osmolality of 250 mOsm/kg (250 mmol/kg):Blood osmolality within the normal range (usually around 275-295 mOsm/kg) is not directly associated with complications of inhibiting aldosterone secretion. Blood osmolality reflects the concentration of solutes in the blood and is regulated by various factors, including water balance, electrolyte levels, and hormonal regulation. Inhibiting aldosterone secretion primarily affects electrolyte balance rather than blood osmolality.
D. Urine output of 25 mL/hr
Urine output of 25 mL/hr:A urine output of 25 mL/hr is considered low and may indicate decreased renal perfusion or impaired kidney function. Inhibiting aldosterone secretion can affect renal function and urine output, leading to decreased urine production. Reduced urine output can contribute to fluid and electrolyte imbalances and may be a concern in patients with inhibited aldosterone secretion.
E. Serum potassium level of 5.4 mEq/L:
A serum potassium level of 5.4 mEq/L indicates hyperkalemia, which is another potential complication of inhibiting aldosterone secretion. Aldosterone helps regulate potassium levels by promoting potassium excretion in the kidneys. When aldosterone secretion is inhibited, potassium excretion decreases, leading to an accumulation of potassium in the bloodstream and resulting in hyperkalemia. Symptoms of hyperkalemia may include muscle weakness, irregular heartbeat, nausea, and numbness or tingling.
Full Explanation
A serum potassium level of 3.2 mEq/L indicates hypokalemia, which is a potential complication of inhibiting aldosterone secretion and release. Aldosterone plays a key role in potassium regulation in the body by promoting potassium excretion in the kidneys. When aldosterone secretion is inhibited, potassium excretion decreases, leading to an accumulation of potassium in the bloodstream and resulting in hypokalemia. Symptoms of hypokalemia may include muscle weakness, cramping, irregular heartbeat, and fatigue.
B. Urine output of 1,200 mL in the last 2 hours:
This option does not directly relate to complications of inhibiting aldosterone secretion. A urine output of 1,200 mL in the last 2 hours indicates adequate urine production, which is generally a positive sign. However, in the context of inhibiting aldosterone secretion, the nurse would be more concerned about decreased urine output due to potential renal effects.
C. Blood osmolality of 250 mOsm/kg (250 mmol/kg):
Blood osmolality within the normal range (usually around 275-295 mOsm/kg) is not directly associated with complications of inhibiting aldosterone secretion. Blood osmolality reflects the concentration of solutes in the blood and is regulated by various factors, including water balance, electrolyte levels, and hormonal regulation. Inhibiting aldosterone secretion primarily affects electrolyte balance rather than blood osmolality.
D. Urine output of 25 mL/hr:
A urine output of 25 mL/hr is considered low and may indicate decreased renal perfusion or impaired kidney function. Inhibiting aldosterone secretion can affect renal function and urine output, leading to decreased urine production. Reduced urine output can contribute to fluid and electrolyte imbalances and may be a concern in patients with inhibited aldosterone secretion.
E. Serum potassium level of 5.4 mEq/L:
A serum potassium level of 5.4 mEq/L indicates hyperkalemia, which is another potential complication of inhibiting aldosterone secretion. Aldosterone helps regulate potassium levels by promoting potassium excretion in the kidneys. When aldosterone secretion is inhibited, potassium excretion decreases, leading to an accumulation of potassium in the bloodstream and resulting in hyperkalemia. Symptoms of hyperkalemia may include muscle weakness, irregular heartbeat, nausea, and numbness or tingling.