Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
Patient Data
History and Physical Nurses' Notes Laboratory Results Flow Sheet
Review H and P, nurse's note, laboratory result, and flow sheet.
What information should the nurse collect as part of the focused assessment for dehydration in this child? Select all that apply.
A. Level of consciousness
Assessing the level of consciousness, pupil size and reactiveness, and respiratory rate are important aspects of the neurological and respiratory assessments but are not specific to the assessment of dehydration
B. Capillary refill
This is a quick and simple way to assess the adequacy of peripheral perfusion and can help identify signs of dehydration.
C. Temperature
Fever is a potential cause of dehydration, so monitoring the temperature is an important part of the assessment.
D. Blood pressure
Blood pressure can be affected by dehydration, so monitoring it is important in determining the severity of dehydration and in guiding appropriate interventions.
F. Pupil size and reactiveness
Assessing the level of consciousness, pupil size and reactiveness, and respiratory rate are important aspects of the neurological and respiratory assessments but are not specific to the assessment of dehydration
G. Skin turgor
Assessing the skin turgor, or the elasticity of the skin, is another useful indicator of dehydration.
H. Heart rate
Tachycardia can be a sign of dehydration, so monitoring the heart rate is an important component of the assessment.
This question is an excerpt from Nurse Dive's nursing test bank - RN Hesi Exit Proctored Exam. Take the full exam now
Full Explanation
- Capillary refill: This is a quick and simple way to assess the adequacy of peripheral perfusion and can help identify signs of dehydration.
- Skin turgor: Assessing the skin turgor, or the elasticity of the skin, is another useful indicator of dehydration.
- Heart rate: Tachycardia can be a sign of dehydration, so monitoring the heart rate is an important component of the assessment.
- Blood pressure: Blood pressure can be affected by dehydration, so monitoring it is important in determining the severity of dehydration and in guiding appropriate interventions.
- Temperature: Fever is a potential cause of dehydration, so monitoring the temperature is an important part of the assessment.
- Skin color of hands and feet: Checking the color of the skin on the hands and feet can help identify signs of poor perfusion and dehydration.
Assessing the level of consciousness, pupil size and reactiveness, and respiratory rate are important aspects of the neurological and respiratory assessments but are not specific to the assessment of dehydration.
Similar Questions
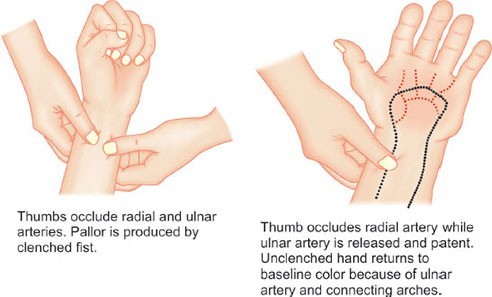
When should the nurse conduct an Allen's test?
A. Just before arterial blood gasses are drawn peripherally.
Allen's test is a procedure used to assess the patency of the ulnar artery and the collateral circulation of the hand. It is performed to determine the adequacy of collateral circulation before obtaining arterial blood gases from the radial artery. The test helps ensure that the ulnar artery is functioning properly and can supply blood to the hand if the radial artery is used for blood sampling or other invasive procedures. The test involves occluding both the ulnar and radial arteries while the patient clenches their fist. The nurse then releases pressure on the ulnar artery while maintaining occlusion of the radial artery. The hand should quickly regain normal coloration, indicating adequate collateral circulation. It's important to note that the Allen's test is specific to the assessment of collateral circulation in the hand and is not used for other purposes such as assessing deep vein thrombosis, cardiac output calculation, or obtaining pulmonary artery pressures.
B. Prior to attempting a cardiac output calculation.
C. To assess for presence of a deep vein thrombus in the leg.
D. When pulmonary artery pressures are obtained.
Full Explanation
Allen's test is a procedure used to assess the patency of the ulnar artery and the collateral circulation of the hand. It is performed to determine the adequacy of collateral circulation before obtaining arterial blood gases from the radial artery. The test helps ensure that the ulnar artery is functioning properly and can supply blood to the hand if the radial artery is used for blood sampling or other invasive procedures.
The test involves occluding both the ulnar and radial arteries while the patient clenches their fist. The nurse then releases pressure on the ulnar artery while maintaining occlusion of the radial artery. The hand should quickly regain normal coloration, indicating adequate collateral circulation.
It's important to note that the Allen's test is specific to the assessment of collateral circulation in the hand and is not used for other purposes such as assessing deep vein thrombosis, cardiac output calculation, or obtaining pulmonary artery pressures.
The nurse is preparing to administer 1.6 mL of medication intramuscularly to a 4-month-old infant. Which action should the nurse include?
A. Select a 22 gauge 1 1/2 inch (3.8 cm) needle for the intramuscular injection.
In addition, the nurse should select an appropriate needle size and injection site based on the infant's size and age. A 22 gauge 1 1/2 inch (3.8 cm) needle is too large for an infant and may cause discomfort and tissue damage. The nurse should use a smaller gauge needle and choose an appropriate injection site, such as the vastus lateralis muscle in the thigh or the dorsogluteal muscle in the buttocks, based on the infant's age and size.
B. Divide the medication into two injections with volumes under 1 mL.
Administering a large volume of medication in a single injection is not recommended for infants as it can lead to discomfort, tissue trauma, and potential complications such as muscle fibrosis or nerve injury. Dividing the medication into two injections with volumes under 1 mL is a common practice for infants and can help minimize discomfort and complications.
C. Administer into the deltoid muscle while the parent holds the infant securely.
Finally, administering an injection into the deltoid muscle is not recommended for infants as this muscle is not fully developed until later in childhood.
D. Use a quick dart-like motion to inject into the dorsogluteal site.
Using a quick dart-like motion to inject into the dorsogluteal site is also not recommended as it can cause tissue damage and discomfort. Instead, the nurse should use a slow, steady technique to administer the injection while ensuring the infant is held securely by the parent or another caregiver.
Full Explanation
Administering a large volume of medication in a single injection is not recommended for infants as it can lead to discomfort, tissue trauma, and potential complications such as muscle fibrosis or nerve injury. Dividing the medication into two injections with volumes under 1 mL is a common practice for infants and can help minimize discomfort and complications.
In addition, the nurse should select an appropriate needle size and injection site based on the infant's size and age. A 22 gauge 1 1/2 inch (3.8 cm) needle is too large for an infant and may cause discomfort and tissue damage. The nurse should use a smaller gauge needle and choose an appropriate injection site, such as the vastus lateralis muscle in the thigh or the dorsogluteal muscle in the buttocks, based on the infant's age and size.
Finally, administering an injection into the deltoid muscle is not recommended for infants as this muscle is not fully developed until later in childhood. Using a quick dart-like motion to inject into the dorsogluteal site is also not recommended as it can cause tissue damage and discomfort. Instead, the nurse should use a slow, steady technique to administer the injection while ensuring the infant is held securely by the parent or another caregiver.
A client is admitted to the surgical intensive care unit following the removal of a large portion of the intestines due to a gunshot wound to the abdomen. The client begins to display signs of septic shock and a sepsis protocol is initiated. Which intervention is most important for the nurse to include in the plan of care?
A. Maintain strict intake and output.
Septic shock is a life-threatening condition characterized by a severe infection that leads to systemic inflammation, organ dysfunction, and low blood pressure. Maintaining strict intake and output monitoring is essential to assess the client's fluid balance and response to interventions. It allows the nurse to closely monitor the client's urine output, which is a crucial indicator of renal perfusion and overall organ function. Monitoring urine output helps the nurse assess the adequacy of tissue perfusion and the client's response to fluid resuscitation. A decrease in urine output can be an early sign of worsening organ dysfunction and a need for further interventions.
B. Assess warmth of extremities.
While assessing the warmth of extremities is important for evaluating peripheral perfusion, maintaining strict intake and output monitoring takes priority as it provides more comprehensive information about the client's overall fluid status.
C. Keep head of bed raised 45 degrees.
Raising the head of the bed 45 degrees (semi-Fowler's position) can help optimize respiratory function and reduce the risk of aspiration, but it is not the most important intervention in this case.Monitoring blood glucose levels is important, as hyperglycemia can be associated with sepsis. However, in the context of septic shock, maintaining strict intake and output monitoring takes precedence as it directly assesses the client's fluid balance and response to interventions.
D. Monitor blood glucose level.
Monitoring blood glucose levels is important, as hyperglycemia can be associated with sepsis. However, in the context of septic shock, maintaining strict intake and output monitoring takes precedence as it directly assesses the client's fluid balance and response to interventions.
Full Explanation
Septic shock is a life-threatening condition characterized by a severe infection that leads to systemic inflammation, organ dysfunction, and low blood pressure. Maintaining strict intake and output monitoring is essential to assess the client's fluid balance and response to interventions. It allows the nurse to closely monitor the client's urine output, which is a crucial indicator of renal perfusion and overall organ function.
Monitoring urine output helps the nurse assess the adequacy of tissue perfusion and the client's response to fluid resuscitation. A decrease in urine output can be an early sign of worsening organ dysfunction and a need for further interventions.
While assessing the warmth of extremities is important for evaluating peripheral perfusion, maintaining strict intake and output monitoring takes priority as it provides more comprehensive information about the client's overall fluid status.
Raising the head of the bed 45 degrees (semi-Fowler's position) can help optimize respiratory function and reduce the risk of aspiration, but it is not the most important intervention in this case.
Monitoring blood glucose levels is important, as hyperglycemia can be associated with sepsis. However, in the context of septic shock, maintaining strict intake and output monitoring takes precedence as it directly assesses the client's fluid balance and response to interventions.
It's crucial to note that the management of septic shock requires a multidisciplinary approach, and other interventions, such as administering appropriate antibiotics, initiating fluid resuscitation, and addressing the underlying source of infection, should also be implemented in a timely manner.