Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The nurse in the women's health clinic has four patients who are waiting to be seen. Which patient should the nurse see first?
A. A 42-yr-old patient with secondary amenorrhea who says that her last menstrual cycle was 3 months ago
The 42-yr-old patient with secondary amenorrhea may have menopause, pregnancy, or a hormonal disorder. This is less urgent compared to the 19- year old patient.
B. A 19-yr-old patient with menorrhagia who has been using superabsorbent tampons and has fever with weakness
This patient may have toxic shock syndrome, which is a life- threatening complication of tampon use that can cause organ failure and shock. The nurse should assess the patient's vital signs, remove the tampon, and initiate fluid resuscitation and antibiotic therapy.
C. A 22-yr-old patient with persistent red-brown vaginal drainage 3 days after having balloon thermotherapy
This patient may have an infection or a complication of the balloon thermotherapy, which is a procedure to destroy the endometrial lining of the uterus and is not an emergency compared to the 19 year old.
D. A 35-yr-old patient with heavy spotting after having a progestin-containing IUD (Mirena) inserted a month ago
This patient may have a displacement or perforation of the IUD, which is a contraceptive device that releases progestin into the uterus. However, this is not urgent compared to the 19 year old.
This question is an excerpt from Nurse Dive's nursing test bank - Interprofessional Care of the Client and Family Across the Lifespan II Proctored Exam. Take the full exam now
Full Explanation
Choice A rationale: The 42-yr-old patient with secondary amenorrhea may have menopause, pregnancy, or a hormonal disorder. This is less urgent compared to the 19- year old patient.
Choice B rationale: This patient may have toxic shock syndrome, which is a life- threatening complication of tampon use that can cause organ failure and shock. The nurse should assess the patient's vital signs, remove the tampon, and initiate fluid resuscitation and antibiotic therapy.
Choice C rationale: This patient may have an infection or a complication of the balloon thermotherapy, which is a procedure to destroy the endometrial lining of the uterus and is not an emergency compared to the 19 year old.
Choice D rationale: This patient may have a displacement or perforation of the IUD, which is a contraceptive device that releases progestin into the uterus. However, this is not urgent compared to the 19 year old.
Similar Questions
The nurse is caring for a client with multiple traumas after a motor vehicle collision.
The nurse learns that the client has secondary syphilis. What precaution should the nurse implement?
A. a Gloves should be worn during direct contact with the client's skin.
Gloves should be worn during direct contact with the client's skin. This is a standard precaution that applies to all clients, but especially to those with infectious diseases that can be transmitted through contact. Secondary syphilis is highly contagious and can be spread through direct contact with the skin lesions or mucous membranes of an infected person.
B. No precautions in addition to standard precautions are necessary.
This is incorrect because secondary syphilis requires more than standard precautions to prevent transmission.
C. Handwashing is required before and after contact with the client.
This is incorrect because handwashing is a basic component of standard precautions and is not sufficient to prevent the spread of syphilis.
D. A mask should be worn by anyone entering the client's room.
This is incorrect because a mask is not necessary for contact precautions, unless the client has respiratory symptoms or is undergoing aerosol- generating procedures.
Full Explanation
Choice A rationale: Gloves should be worn during direct contact with the client's skin. This is a standard precaution that applies to all clients, but especially to those with infectious diseases that can be transmitted through contact. Secondary syphilis is highly contagious and can be spread through direct contact with the skin lesions or mucous
membranes of an infected person.
Choice B rationale: This is incorrect because secondary syphilis requires more than standard precautions to prevent transmission.
Choice C rationale: This is incorrect because handwashing is a basic component of standard precautions and is not sufficient to prevent the spread of syphilis.
Choice D rationale: This is incorrect because a mask is not necessary for contact precautions, unless the client has respiratory symptoms or is undergoing aerosol- generating procedures.
A client with a 16-year history of diabetes mellitus is having renal function tests because of recent fatigue, weakness, elevated blood urea nitrogen, and serum creatinine levels. Which finding should the nurse conclude as an early symptom of renal insufficiency?
A. Stomatitis and Diarrhea
These are symptoms of advance renal failure. Stomatitis and diarrhea are signs of uremia, which is the accumulation of waste products in the blood.
B. Dyspnea and Anuria
Dyspnea and anuria are signs of fluid overload and kidney shutdown and indicate advanced renal failure.
C. Confusion and Vomiting
Confusion and vomiting are signs of acidosis and electrolyte disturbances and occur in advanced stages of renal failure.
D. Nocturia and Oliguria
One of the early symptoms of renal insufficiency is nocturia, which is the need to urinate frequently at night. This occurs because the kidneys are unable to concentrate urine during the day and produce more urine at night. Another early symptom is oliguria, which is the production of less than 400 mL of urine per day. This occurs because the kidneys are unable to excrete enough urine to maintain fluid balance.
Full Explanation
Choice A rationale: These are symptoms of advance renal failure. Stomatitis and diarrhea are signs of uremia, which is the accumulation of waste products in the blood.
Choice B rationale: Dyspnea and anuria are signs of fluid overload and kidney shutdown and indicate advanced renal failure.
Choice C rationale: Confusion and vomiting are signs of acidosis and electrolyte disturbances and occur in advanced stages of renal failure.
Choice D rationale: One of the early symptoms of renal insufficiency is nocturia, which is the need to urinate frequently at night. This occurs because the kidneys are unable to concentrate urine during the day and produce more urine at night. Another early symptom is oliguria, which is the production of less than 400 mL of urine per day. This occurs because the kidneys are unable to excrete enough urine to maintain fluid balance.
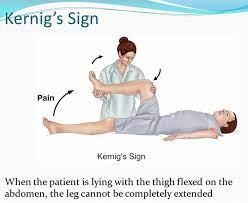
Which of the following describes the correct procedure for testing for Kernig's sign?
A. Rotate the neck to one side while observing the eyes moving to the opposite side.
Rotating the neck to one side while observing the eyes moving to the opposite side is a procedure for testing for oculocephalic reflex or doll's eye phenomenon, which indicates brainstem function.
B. Passively elevate the leg with extended knee while observing for pain, resistance, or flexion.
This is the correct answer. Kernig's sign is a clinical sign that indicates meningitis, which is an inflammation of the membranes that cover the brain and spinal cord. To test for Kernig's sign, the nurse should flex the patient's hip to 90 degrees and then attempt to extend the knee. A positive Kernig's sign is when the patient experiences pain in the lower back or hamstring, resists knee extension, or involuntarily flexes the opposite leg.
C. Stroke the lateral aspect of the sole of the patient's foot and observe for dorsiflexion of the big toe.
Stroking the lateral aspect of the sole of the patient's foot and observing for dorsiflexion of the big toe is a procedure for testing for Babinski's sign, which indicates upper motor neuron lesion or damage.
D. Passively flex the patient's neck forward and observe for hip and knee flexion.
Passively flexing the patient's neck forward and observing for hip and knee flexion is a procedure for testing for Brudzinski's sign, which also indicates meningitis.
Full Explanation
Choice A rationale: Rotating the neck to one side while observing the eyes moving to the opposite side is a procedure for testing for oculocephalic reflex or doll's eye
phenomenon, which indicates brainstem function.
Choice B rationale: This is the correct answer. Kernig's sign is a clinical sign that indicates meningitis, which is an inflammation of the membranes that cover the brain and spinal cord. To test for Kernig's sign, the nurse should flex the patient's hip to 90 degrees and then attempt to extend the knee. A positive Kernig's sign is when the patient
experiences pain in the lower back or hamstring, resists knee extension, or involuntarily flexes the opposite leg.
Choice C rationale: Stroking the lateral aspect of the sole of the patient's foot and observing for dorsiflexion of the big toe is a procedure for testing for Babinski's sign, which indicates upper motor neuron lesion or damage.
Choice D rationale: Passively flexing the patient's neck forward and observing for hip and knee flexion is a procedure for testing for Brudzinski's sign, which also indicates meningitis.
 |