Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The nurse is caring for a client who has a bowel obstruction and a new prescription for the insertion of a nasogastric tube. Which of the following interventions should the nurse take when inserting the nasogastric tube?
A. Measure the tube for insertion from the tip of the nose to the umbilicus.
Choice A: Measure the tube for insertion from the tip of the nose to the umbilicus. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should measure the tube for insertion from the tip of the nose to the earlobe and then to the xiphoid process, which is a more accurate way of estimating the length of the tube needed to reach the stomach.
B. Place the client in a supine position.
Choice B: Place the client in a supine position. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should place the client in a high-Fowler’s position, which is a position with the head of the bed elevated to 90 degrees. This position can prevent aspiration, promote breathing, and allow gravity to assist with the insertion of the tube.
C. Withdraw the tube if the client gags during insertion.
Choice C: Withdraw the tube if the client gags during insertion. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should not withdraw the tube if the client gags during insertion, as this can cause trauma to the nasal or pharyngeal mucosa and increase discomfort. The nurse should pause and allow the client to rest and breathe until gagging subsides, then resume insertion. The nurse should also provide reassurance and encouragement to the client throughout the procedure.
D. Instruct the client to place his chin to his chest and swallow.
Choice D: Instruct the client to place his chin to his chest and swallow. This is an intervention that the nurse should take when inserting a nasogastric tube, which is a flexible tube that is inserted through the nose and into the stomach. The nurse should instruct the client to place his chin to his chest and swallow as the tube passes through the pharynx and into the esophagus. This can facilitate the insertion of the tube and prevent it from entering the trachea or causing injury to the nasal or pharyngeal mucosa.
This question is an excerpt from Nurse Dive's nursing test bank - ATI LPN Med Surg Proctored Exam. Take the full exam now
Full Explanation
Choice A: Measure the tube for insertion from the tip of the nose to the umbilicus. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should measure the tube for insertion from the tip of the nose to the earlobe and then to the xiphoid process, which is a more accurate way of estimating the length of the tube needed to reach the stomach.
Choice B: Place the client in a supine position. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should place the client in a high-Fowler’s position, which is a position with the head of the bed elevated to 90 degrees. This position can prevent aspiration, promote breathing, and allow gravity to assist with the insertion of the tube.
Choice C: Withdraw the tube if the client gags during insertion. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should not withdraw the tube if the client gags during insertion, as this can cause trauma to the nasal or pharyngeal mucosa and increase discomfort. The nurse should pause and allow the client to rest and breathe until gagging subsides, then resume insertion. The nurse should also provide reassurance and encouragement to the client throughout the procedure.
Choice D: Instruct the client to place his chin to his chest and swallow. This is an intervention that the nurse should take when inserting a nasogastric tube, which is a flexible tube that is inserted through the nose and into the stomach. The nurse should instruct the client to place his chin to his chest and swallow as the tube passes through the pharynx and into the esophagus. This can facilitate the insertion of the tube and prevent it from entering the trachea or causing injury to the nasal or pharyngeal mucosa.
Similar Questions
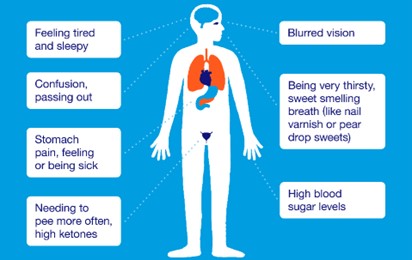
A nurse is collecting data from a client who has diabetes mellitus. Which of the following findings indicates that the client is experiencing DKA?
A. Rapid pulse
Choice A: Rapid pulse. This is not a finding that indicates that the client is experiencing DKA, but rather a sign of hypoglycemia, which is a low level of glucose in the blood. Hypoglycemia can cause rapid pulse due to increased sympathetic nervous system activity and decreased cardiac output.
B. Clammy skin
Choice B: Clammy skin. This is not a finding that indicates that the client is experiencing DKA, but rather a sign of hypoglycemia. Hypoglycemia can cause clammy skin due to increased sweating and vasoconstriction.
C. Confusion
Choice C: Confusion is commonly found in HHS rather than DKA.
D. Polydipsia
Choice D: Polydipsia. This is a finding that indicates that the client is experiencing DKA due to the high level of glucose in the blood. Hyperglycemia in DKA can cause polydipsia, which is excessive thirst, due to osmotic diuresis and dehydration.
Full Explanation
Choice A: Rapid pulse. This is not a finding that indicates that the client is experiencing DKA, but rather a sign of hypoglycemia, which is a low level of glucose in the blood. Hypoglycemia can cause rapid pulse due to increased sympathetic nervous system activity and decreased cardiac output.
Choice B: Clammy skin. This is not a finding that indicates that the client is experiencing DKA, but rather a sign of hypoglycemia. Hypoglycemia can cause clammy skin due to increased sweating and vasoconstriction.
Choice C: Choice C: Confusion is commonly found in HHS rather than DKA.
Choice D: Polydipsia. This is a finding that indicates that the client is experiencing DKA due to the high level of glucose in the blood. Hyperglycemia in DKA can cause polydipsia, which is excessive thirst, due to osmotic diuresis and dehydration.
A nurse is caring for a client who has hyperparathyroidism. Based on this diagnosis, the nurse should monitor the client for which of the following complications?
A. Dysphagia
Choice A: Dysphagia. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Dysphagia is difficulty swallowing, which can be caused by disorders of the esophagus, throat, or nervous system. It is not related to hyperparathyroidism or calcium and phosphorus levels.
B. Pathologic fractures
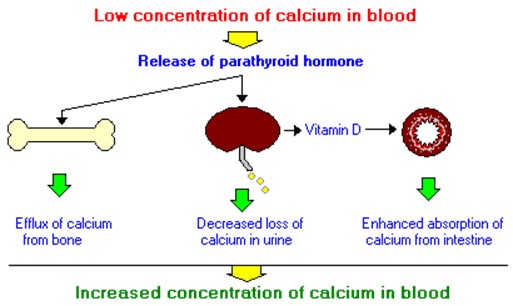
Choice B: Pathologic fractures. This is a complication that the nurse should monitor the client for who has hyperparathyroidism, which is a condition that occurs when the parathyroid glands produce too much parathyroid hormone (PTH). PTH regulates calcium and phosphorus levels in the blood and bones. Hyperparathyroidism can cause hypercalcemia, which is a high level of calcium in the blood, and hypophosphatemia, which is a low level of phosphorus in the blood. These imbalances can lead to bone resorption, which is the breakdown of bone tissue and release of calcium into the blood. Bone resorption can weaken the bones and increase the risk of pathologic fractures, which are fractures that occur due to disease or injury to the bone.
C. Fluid retention
Choice C: Fluid retention. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Fluid retention is excess fluid accumulation in the body, which can be caused by disorders of the heart, kidney, liver, or lymphatic system. It is not related to hyperparathyroidism or calcium and phosphorus levels.
D. Impaired skin integrity
Choice D: Impaired skin integrity. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Impaired skin integrity is damage or loss of skin tissue, which can be caused by trauma, infection, inflammation, or pressure. It is not related to hyperparathyroidism or calcium and phosphorus levels.
Full Explanation
Choice A: Dysphagia. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Dysphagia is difficulty swallowing, which can be caused by disorders of the esophagus, throat, or nervous system. It is not related to hyperparathyroidism or calcium and phosphorus levels.
Choice B: Pathologic fractures. This is a complication that the nurse should monitor the client for who has hyperparathyroidism, which is a condition that occurs when the parathyroid glands produce too much parathyroid hormone (PTH). PTH regulates calcium and phosphorus levels in the blood and bones. Hyperparathyroidism can cause hypercalcemia, which is a high level of calcium in the blood, and hypophosphatemia, which is a low level of phosphorus in the blood. These imbalances can lead to bone resorption, which is the breakdown of bone tissue and release of calcium into the blood. Bone resorption can weaken the bones and increase the risk of pathologic fractures, which are fractures that occur due to disease or injury to the bone.
Choice C: Fluid retention. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Fluid retention is excess fluid accumulation in the body, which can be caused by disorders of the heart, kidney, liver, or lymphatic system. It is not related to hyperparathyroidism or calcium and phosphorus levels.
Choice D: Impaired skin integrity. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Impaired skin integrity is damage or loss of skin tissue, which can be caused by trauma, infection, inflammation, or pressure. It is not related to hyperparathyroidism or calcium and phosphorus levels.
A nurse is caring for a client who is postoperative and has a history of Addison’s disease. For which of the following manifestations should the nurse monitor?
A. Hypernatremia
Choice A: Hypernatremia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Hypernatremia is a high level of sodium in the blood, which can be caused by dehydration, excessive sodium intake, or kidney dysfunction. It is not related to Addison’s disease or cortisol and aldosterone levels.
B. Bradycardia
Choice B: Bradycardia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Bradycardia is a slow heart rate, which can be caused by vagal stimulation, medication side effects, or cardiac disorders. It is not related to Addison’s disease or cortisol and aldosterone levels.
C. Hypotension
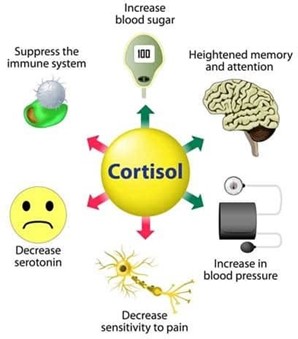
Choice C: Hypotension. This is a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease, which is a condition that occurs when the adrenal glands do not produce enough cortisol and aldosterone. Cortisol is a hormone that regulates the metabolism of carbohydrates, proteins, and fats, and helps the body cope with stress. Aldosterone is a hormone that regulates the balance of sodium and potassium in the blood and fluid volume. Addison’s disease can cause hypotension, which is a low blood pressure, due to decreased aldosterone production and fluid loss.
D. Hypokalemia
Choice D: Hypokalemia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Hypokalemia is a low level of potassium in the blood, which can be caused by diuretics, vomiting, diarrhea, or alkalosis. It is not related to Addison’s disease or cortisol and aldosterone levels.
Full Explanation
Choice A: Hypernatremia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Hypernatremia is a high level of sodium in the blood, which can be caused by dehydration, excessive sodium intake, or kidney dysfunction. It is not related to Addison’s disease or cortisol and aldosterone levels.
Choice B: Bradycardia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Bradycardia is a slow heart rate, which can be caused by vagal stimulation, medication side effects, or cardiac disorders. It is not related to Addison’s disease or cortisol and aldosterone levels.
Choice C: Hypotension. This is a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease, which is a condition that occurs when the adrenal glands do not produce enough cortisol and aldosterone. Cortisol is a hormone that regulates the metabolism of carbohydrates, proteins, and fats, and helps the body cope with stress. Aldosterone is a hormone that regulates the balance of sodium and potassium in the blood and fluid volume. Addison’s disease can cause hypotension, which is a low blood pressure, due to decreased aldosterone production and fluid loss.
Choice D: Hypokalemia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Hypokalemia is a low level of potassium in the blood, which can be caused by diuretics, vomiting, diarrhea, or alkalosis. It is not related to Addison’s disease or cortisol and aldosterone levels.