Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
The practical nurse (PN) notices that one of the unlicensed assistive personnel (UAP) working in the long- term care facility consistently records subnormal temperatures when using a tympanic thermometer.
Which action should the PN take first?
A. Demonstrate how to use the equipment
This is not the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Demonstrating how to use the equipment may be helpful, but it should be done after observing how the UAP obtains temperatures and determining the cause of the discrepancy.
B. Observe how UAP obtains temperatures
This is the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Observing how the UAP obtains temperatures will help the PN identify any errors or problems with the technique, equipment, or documentation. The PN can then provide feedback and guidance to the UAP to ensure accurate and reliable temperature measurements.
C. Show UAP how to chart temperatures
This is not the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Showing UAP how to chart temperatures may be necessary, but it should be done after observing how the UAP obtains temperatures and verifying the accuracy of the data.
D. Return the thermometer for recalibration
This is not the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Returning the thermometer for recalibration may be required, but it should be done after observing how the UAP obtains temperatures and ruling out any human or environmental factors that may affect the readings.
This question is an excerpt from Nurse Dive's nursing test bank - HESI PN Exit 2023 II Proctored Exam. Take the full exam now
Full Explanation
b) Observe how UAP obtains temperatures - Correct Answer
This is the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Observing how the UAP obtains temperatures will help the PN identify any errors or problems with the technique, equipment, or documentation. The PN can then provide feedback and guidance to the UAP to ensure accurate and reliable temperature measurements.
a) Demonstrate how to use the equipment.
This is not the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Demonstrating how to use the equipment may be helpful, but it should be done after observing how the UAP obtains temperatures and determining the cause of the discrepancy.
c) Show UAP how to chart temperatures.
This is not the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Showing UAP how to chart temperatures may be necessary, but it should be done after observing how the UAP obtains temperatures and verifying the accuracy of the data.
d) Return the thermometer for recalibration.
This is not the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Returning the thermometer for recalibration may be required, but it should be done after observing how the UAP obtains temperatures and ruling out any human or environmental factors that may affect the readings.
Similar Questions
An adult female client with type 1 diabetes mellitus is receiving NPH insulin 35 units each morning. Which finding should the practical nurse (PN) document as evidence that the amount of insulin is inadequate?
A. States her feet are constantly cold along with feeling numb
This is not the finding that the PN should document as evidence that the amount of insulin is inadequate for the client with type 1 diabetes mellitus. States her feet are constantly cold along with feeling numb may indicate peripheral neuropathy, which is a complication of diabetes that affects the nerves in the feet and legs. It is caused by chronic high blood sugar levels over time, not by a single dose of insulin.
B. Consecutive evening serum glucose greater than 260 mg/dL
This is the finding that the PN should document as evidence that the amount of insulin is inadequate for the client with type 1 diabetes mellitus. Consecutive evening serum glucose greater than 260 mg/dL indicates hyperglycemia, which means that the client's blood sugar is too high and not well controlled by the insulin dose. The PN should report this finding to the healthcare provider and expect a possible adjustment in the insulin regimen.
C. A wound on the ankle that starts to drain and becomes painful
This is not the finding that the PN should document as evidence that the amount of insulin is inadequate for the client with type 1 diabetes mellitus. A wound on the ankle that starts to drain and becomes painful may indicate an infection, which is a risk factor for diabetic clients due to impaired wound healing and immune function. It is not directly related to the insulin dose, although it may affect the blood sugar levels and require more insulin.
D. Reports nausea in the morning but still able to eat breakfast
This is not the finding that the PN should document as evidence that the amount of insulin is inadequate for the client with type 1 diabetes mellitus. Reports nausea in the morning but still able to eat breakfast may indicate morning sickness, which is a common symptom of pregnancy. It is not related to the insulin dose, although it may affect the blood sugar levels and require more frequent monitoring and adjustment.
Full Explanation
The correct answer and explanation is:
b) Consecutive evening serum glucose greater than 260 mg/dL.
This is the finding that the PN should document as evidence that the amount of insulin is inadequate for the client with type 1 diabetes mellitus. Consecutive evening serum glucose greater than 260 mg/dL indicates hyperglycemia, which means that the client's blood sugar is too high and not well controlled by the insulin dose.
The PN should report this finding to the healthcare provider and expect a possible adjustment in the insulin regimen.
a) States her feet are constantly cold along with feeling numb.
This is not the finding that the PN should document as evidence that the amount of insulin is inadequate for the client with type 1 diabetes mellitus.
States her feet are constantly cold along with feeling numb may indicate peripheral neuropathy, which is a complication of diabetes that affects the nerves in the feet and legs. It is caused by chronic high blood sugar levels over time, not by a single dose of insulin.
c) A wound on the ankle that starts to drain and becomes painful.
This is not the finding that the PN should document as evidence that the amount of insulin is inadequate for the client with type 1 diabetes mellitus. A wound on the ankle that starts to drain and becomes painful may indicate an infection, which is a risk factor for diabetic clients due to impaired wound healing and immune function. It is not directly related to the insulin dose, although it may affect the blood sugar levels and require more insulin.
d) Reports nausea in the morning but still able to eat breakfast.
This is not the finding that the PN should document as evidence that the amount of insulin is inadequate for the client with type 1 diabetes mellitus. Reports nausea in the morning but still able to eat breakfast may indicate morning sickness, which is a common symptom of pregnancy. It is not related to the insulin dose, although it may affect the blood sugar levels and require more frequent monitoring and adjustment.

The practical nurse (PN) should collect the following information during the admission assessment of a terminally ill client to an acute care facility:
A. Health care proxy documentation
This is the information that the PN should collect during the admission assessment of a terminally ill client to an acute care facility. Health care proxy documentation is a legal document that appoints a person to make health care decisions for the client when they are unable to do so themselves. It is important to have this information in case the client's condition deteriorates and they need end-of-life care.
B. Name of funeral home to contact
This is not the information that the PN should collect during the admission assessment of a terminally ill client to an acute care facility. Name of funeral home to contact is a personal preference that may or may not be relevant for the client at this point. It is not a priority for the admission assessment, and it may be insensitive or inappropriate to ask the client about it.
C. Client's wishes regarding organ donation
This is not the information that the PN should collect during the admission assessment of a terminally ill client to an acute care facility. Client's wishes regarding organ donation are a personal choice that may or may not be applicable for the client depending on their diagnosis, prognosis, and eligibility. It is not a priority for the admission assessment, and it may be offensive or upsetting to ask the client about it.
D. Contact information for the client's next of kin
This is not the information that the PN should collect during the admission assessment of a terminally ill client to an acute care facility. Contact information for the client's next of kin is a general demographic data that may or may not be relevant for the client's care. It is not a priority for the admission assessment, and it may be already available in the client's records.
Full Explanation
The correct answer and explanation is:
a) Health care proxy documentation.
This is the information that the PN should collect during the admission assessment of a terminally ill client to an acute care facility. Health care proxy documentation is a legal document that appoints a person to make health care decisions for the client when they are unable to do so themselves. It is important to have this information in case the client's condition deteriorates and they need end-of-life care.
b) Name of funeral home to contact.
This is not the information that the PN should collect during the admission assessment of a terminally ill client to an acute care facility. Name of funeral home to contact is a personal preference that may or may not be relevant for the client at this point. It is not a priority for the admission assessment, and it may be insensitive or inappropriate to ask the client about it.
c) Client's wishes regarding organ donation.
This is not the information that the PN should collect during the admission assessment of a terminally ill client to an acute care facility. Client's wishes regarding organ donation are a personal choice that may or may not be applicable for the client depending on their diagnosis, prognosis, and eligibility. It is not a priority for the admission assessment, and it may be offensive or upsetting to ask the client about it.
d) Contact information for the client's next of kin.
This is not the information that the PN should collect during the admission assessment of a terminally ill client to an acute care facility. Contact information for the client's next of kin is a general demographic data that may or may not be relevant for the client's care. It is not a priority for the admission assessment, and it may be already available in the client's records.
 |
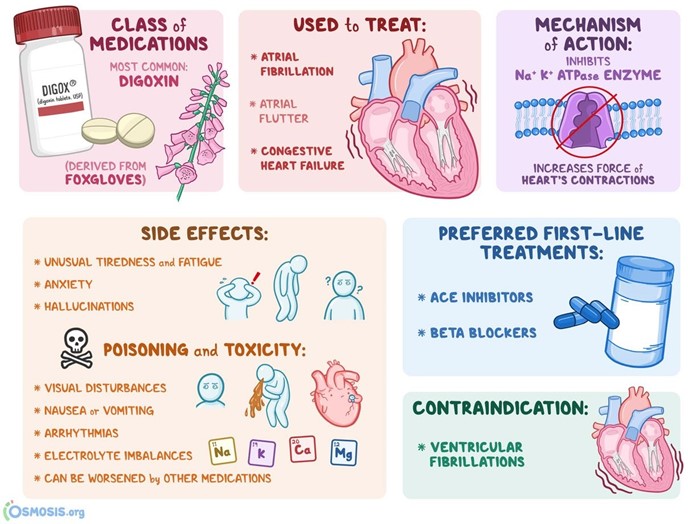
Prior to giving digoxin, the practical nurse (PN) assesses that a 2-month-old infant's heart rate is 120 beats/minute. Based on this, what action should the PN take?
A. Administer the medication and alert the charge nurse
This is not the action that the PN should take prior to giving digoxin to a 2-month-old infant whose heart rate is 120 beats/minute. Alerting the charge nurse is not necessary, as the heart rate is normal and does not indicate a problem with the medication or the client's condition. The PN should administer the medication as prescribed and document the heart rate and any other relevant findings.
B. Hold the medication and document cardiac assessment
This is not the action that the PN should take prior to giving digoxin to a 2-month-old infant whose heart rate is 120 beats/minute. Holding the medication is not appropriate, as the heart rate is normal and does not indicate a contraindication or a risk of adverse effects from the medication. The PN should administer the medication as prescribed and document the heart rate and any other relevant findings.
C. Administer the medication and document the heart rate
This is the action that the PN should take prior to giving digoxin to a 2-month-old infant whose heart rate is 120 beats/minute. Digoxin is a cardiac glycoside that is used to treat heart failure and arrhythmias. It has a narrow therapeutic range and can cause serious side effects such as bradycardia, hypotension, and toxicity. Therefore, it is important to monitor the client's vital signs before and after administering the medication. A normal heart rate for a 2-month-old infant is 100–190 beats/minute, so 120 beats/minute is within the normal range and does not indicate a need to hold the medication. The PN should administer the medication as prescribed and document the heart rate and any other relevant findings.
D. Hold the medication and recheck the heart rate in 1 hour
This is not the action that the PN should take prior to giving digoxin to a 2-month-old infant whose heart rate is 120 beats/minute. Holding the medication and rechecking the heart rate in 1 hour is not necessary, as the heart rate is normal and does not indicate a need for further evaluation or intervention. The PN should administer the medication as prescribed and document the heart rate and any other relevant findings.
Full Explanation
The correct answer and explanation is:
c) Administer the medication and document the heart rate.
This is the action that the PN should take prior to giving digoxin to a 2-month-old infant whose heart rate is 120 beats/minute. Digoxin is a cardiac glycoside that is used to treat heart failure and arrhythmias. It has a narrow therapeutic range and can cause serious side effects such as bradycardia, hypotension, and toxicity. Therefore, it is important to monitor the client's vital signs before and after administering the medication. A normal heart rate for a 2-month-old infant is 100–190 beats/minute, so 120 beats/minute is within the normal range and does not indicate a need to hold the medication. The PN should administer the medication as prescribed and document the heart rate and any other relevant findings.
a) Administer the medication and alert the charge nurse.
This is not the action that the PN should take prior to giving digoxin to a 2-month-old infant whose heart rate is 120 beats/minute. Alerting the charge nurse is not necessary, as the heart rate is normal and does not indicate a problem with the medication or the client's condition. The PN should administer the medication as prescribed and document the heart rate and any other relevant findings.
b) Hold the medication and document cardiac assessment.
This is not the action that the PN should take prior to giving digoxin to a 2-month-old infant whose heart rate is 120 beats/minute. Holding the medication is not appropriate, as the heart rate is normal and does not indicate a contraindication or a risk of adverse effects from the medication. The PN should administer the medication as prescribed and document the heart rate and any other relevant findings.
d) Hold the medication and recheck the heart rate in 1 hour.
This is not the action that the PN should take prior to giving digoxin to a 2-month-old infant whose heart rate is 120 beats/minute. Holding the medication and rechecking the heart rate in 1 hour is not necessary, as the heart rate is normal and does not indicate a need for further evaluation or intervention. The PN should administer the medication as prescribed and document the heart rate and any other relevant findings.
 |