Nursing practice questions with comprehensive rationales
NurseDive Free Nursing Practice Question
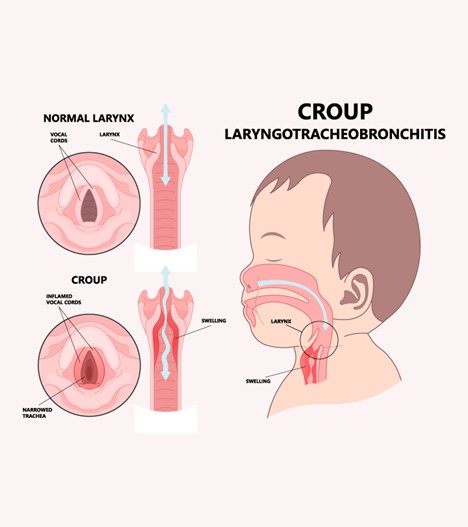
What distinguishing manifestation of spasmodic croup should parents be taught to identify?
A. The child has a high fever.
Spasmodic croup is characterized by sudden-onset symptoms, including a barking cough, but it is not typically associated with a high fever. The barky cough is caused by inflammation and narrowing of the upper airways, leading to a distinct sound when the child coughs.
B. It has a harsh, barky cough.
A harsh, barky cough is a hallmark symptom of spasmodic croup. It is caused by the swelling of the vocal cords and the upper airway, resulting in the characteristic sound. This type of croup is often triggered by viral infections and is usually not bacterial in nature.
C. It is bacterial in nature.
Spasmodic croup is usually of viral origin rather than bacterial. Bacterial infections may lead to other respiratory conditions, but they are not a distinguishing feature of spasmodic croup.
D. Wheezing is heard audibly.
Wheezing is not a typical manifestation of spasmodic croup. Wheezing is often associated with lower airway conditions such as asthma, while croup primarily affects the upper airways and vocal cords, leading to the barking cough.
This question is an excerpt from Nurse Dive's nursing test bank - Pediatrics Midterm V1 2023 Test 3 Proctored Exam. Take the full exam now
Full Explanation
The correct answer is choice B. It has a harsh, barky cough.
Choice A rationale:
Spasmodic croup is characterized by sudden-onset symptoms, including a barking cough, but it is not typically associated with a high fever. The barky cough is caused by inflammation and narrowing of the upper airways, leading to a distinct sound when the child coughs.
Choice B rationale:
A harsh, barky cough is a hallmark symptom of spasmodic croup. It is caused by the swelling of the vocal cords and the upper airway, resulting in the characteristic sound. This type of croup is often triggered by viral infections and is usually not bacterial in nature.
Choice C rationale:
Spasmodic croup is usually of viral origin rather than bacterial. Bacterial infections may lead to other respiratory conditions, but they are not a distinguishing feature of spasmodic croup.
Choice D rationale:
Wheezing is not a typical manifestation of spasmodic croup. Wheezing is often associated with lower airway conditions such as asthma, while croup primarily affects the upper airways and vocal cords, leading to the barking cough.
Similar Questions
Which structural defects constitute tetralogy of Fallot?
A. Pulmonic stenosis, ventricular septal defect, aortic hypertrophy, left ventricular hypertrophy.
Pulmonic stenosis, ventricular septal defect, aortic hypertrophy, left ventricular hypertrophy. This choice is incorrect because it includes "aortic hypertrophy" and "left ventricular hypertrophy," which are not components of the tetralogy of Fallot. Aortic hypertrophy is not a recognized structural defect in tetralogy of Fallot, and left ventricular hypertrophy is not a characteristic feature of this congenital heart condition.
B. Pulmonic stenosis, ventricular septal defect, overriding aorta, right ventricular hypertrophy.
Pulmonic stenosis, ventricular septal defect, overriding aorta, right ventricular hypertrophy. This is the correct choice. Tetralogy of Fallot is characterized by four specific structural defects: pulmonic stenosis (narrowing of the pulmonary valve), ventricular septal defect (hole between the right and left ventricles), overriding aorta (aorta positioned over the ventricular septal defect, receiving blood from both ventricles), and right ventricular hypertrophy (enlargement of the right ventricle due to increased workload).
C. Aortic stenosis, ventricular septal defect, overriding aorta, right ventricular hypertrophy.
Aortic stenosis, ventricular septal defect, overriding aorta, right ventricular hypertrophy. This choice is incorrect because it includes "aortic stenosis," which is not part of the tetralogy of Fallot. In tetralogy of Fallot, the stenosis occurs at the pulmonary valve, not the aortic valve.
D. Aortic stenosis, atrial septal defect, overriding aorta, left ventricular hypertrophy.
Aortic stenosis, atrial septal defect, overriding aorta, left ventricular hypertrophy. This choice is incorrect. While "overriding aorta" is present in tetralogy of Fallot, "atrial septal defect" and "left ventricular hypertrophy" are not part of this condition. Atrial septal defects involve a hole between the two atria, not the ventricles, and left ventricular hypertrophy is not typically seen in tetralogy of Fallot.
Full Explanation
The correct answer is choice B: Pulmonic stenosis, ventricular septal defect, overriding aorta, right ventricular hypertrophy.
Choice A rationale:
Pulmonic stenosis, ventricular septal defect, aortic hypertrophy, left ventricular hypertrophy. This choice is incorrect because it includes "aortic hypertrophy" and "left ventricular hypertrophy," which are not components of the tetralogy of Fallot. Aortic hypertrophy is not a recognized structural defect in tetralogy of Fallot, and left ventricular hypertrophy is not a characteristic feature of this congenital heart condition.
Choice B rationale:
Pulmonic stenosis, ventricular septal defect, overriding aorta, right ventricular hypertrophy. This is the correct choice. Tetralogy of Fallot is characterized by four specific structural defects: pulmonic stenosis (narrowing of the pulmonary valve), ventricular septal defect (hole between the right and left ventricles), overriding aorta (aorta positioned over the ventricular septal defect, receiving blood from both ventricles), and right ventricular hypertrophy (enlargement of the right ventricle due to increased workload).
Choice C rationale:
Aortic stenosis, ventricular septal defect, overriding aorta, right ventricular hypertrophy. This choice is incorrect because it includes "aortic stenosis," which is not part of the tetralogy of Fallot. In tetralogy of Fallot, the stenosis occurs at the pulmonary valve, not the aortic valve.
Choice D rationale:
Aortic stenosis, atrial septal defect, overriding aorta, left ventricular hypertrophy. This choice is incorrect. While "overriding aorta" is present in tetralogy of Fallot, "atrial septal defect" and "left ventricular hypertrophy" are not part of this condition. Atrial septal defects involve a hole between the two atria, not the ventricles, and left ventricular hypertrophy is not typically seen in tetralogy of Fallot.
The nurse is caring for a school-age girl who has had a cardiac catheterization. The child tells the nurse that her bandage is "too wet." The nurse finds the bandage and bed soaked with blood. What is the most appropriate initial nursing action?
A. Place the child in the Trendelenburg position.
is wrong because placing the child in the Trendelenburg position is not an appropriate initial nursing action in this scenario. This position can increase intracranial pressure and is typically used for patients experiencing shock or hypotension.
B. Apply a new bandage with more pressure.
is wrong because applying a new bandage with more pressure might be a subsequent action, but the priority is to apply direct pressure to slow down the bleeding.
C. Notify the physician.
is wrong because notifying the physician is important, but the nurse should first take immediate action to control the bleeding and minimize potential harm to the patient.
D. Apply direct pressure above the catheterization site.
The first action should be to apply direct pressure above the catheterization site to help control the bleeding and minimize blood loss. This will also give the nurse time to prepare additional interventions or supplies if necessary.
Full Explanation
Answer is: d. Apply direct pressure above the catheterization site.
Explanation: The first action should be to apply direct pressure above the catheterization site to help control the bleeding and minimize blood loss. This will also give the nurse time to prepare additional interventions or supplies if necessary.
Choice a. is wrong because placing the child in the Trendelenburg position is not an appropriate initial nursing action in this scenario. This position can increase intracranial pressure and is typically used for patients experiencing shock or hypotension.
Choice b. is wrong because applying a new bandage with more pressure might be a subsequent action, but the priority is to apply direct pressure to slow down the bleeding.
Choice c. is wrong because notifying the physician is important, but the nurse should first take immediate action to control the bleeding and minimize potential harm to the patient.
Pancreatic enzymes are administered to the child with cystic fibrosis. What information should be included in patient education concerning the administration of these enzymes?
A. Administer pancreatic enzymes between meals if at all possible.
Administer pancreatic enzymes between meals if at all possible. This is the correct choice. When educating the parents and child with cystic fibrosis about the administration of pancreatic enzymes, it's important to emphasize that these enzymes should be given between meals whenever feasible. Administering them between meals, when the stomach is less acidic and less likely to release the enzymes prematurely, ensures optimal digestion of food and absorption of nutrients. This approach aligns with the physiological need to supplement pancreatic enzyme function due to the inadequate natural enzyme production in cystic fibrosis.
B. Pancreatic enzymes can be swallowed whole or sprinkled on a small amount of food taken at the beginning of a meal.
Pancreatic enzymes can be swallowed whole or sprinkled on a small amount of food taken at the beginning of a meal. This choice is a valid option for administering pancreatic enzymes. While it's true that the enzymes can be taken either by swallowing the capsules whole or by opening them and sprinkling the contents on a small amount of food at the start of a meal, this method can vary based on individual preferences and abilities. However, the primary focus should be on timing (between meals) to achieve the best enzymatic action.
C. Do not administer pancreatic enzymes if the child is receiving antibiotics.
Do not administer pancreatic enzymes if the child is receiving antibiotics. This statement is not accurate. There is no general contraindication to administering pancreatic enzymes while a child is on antibiotics. However, it's important for the healthcare provider to be aware of all the medications the child is taking to ensure there are no potential drug interactions or effects on absorption. Always consult with the healthcare team before adjusting the administration of any medication.
D. Decrease the dose of pancreatic enzymes if the child is having frequent, bulky stools.
Decrease the dose of pancreatic enzymes if the child is having frequent, bulky stools. This statement is not consistent with typical practice. If a child is experiencing frequent, bulky stools, it may actually indicate that the pancreatic enzyme dosage needs adjustment (increasing the dose rather than decreasing). Bulky stools can suggest poor digestion and absorption, which might require more enzymes to properly break down nutrients. Dosage adjustments should always be made under the guidance of the healthcare provider based on factors such as stool consistency, weight gain, and nutritional status.
Full Explanation
The correct answer is choice A: Administer pancreatic enzymes between meals if at all possible.
Choice A rationale:
Administer pancreatic enzymes between meals if at all possible. This is the correct choice. When educating the parents and child with cystic fibrosis about the administration of pancreatic enzymes, it's important to emphasize that these enzymes should be given between meals whenever feasible. Administering them between meals, when the stomach is less acidic and less likely to release the enzymes prematurely, ensures optimal digestion of food and absorption of nutrients. This approach aligns with the physiological need to supplement pancreatic enzyme function due to the inadequate natural enzyme production in cystic fibrosis.
Choice B rationale:
Pancreatic enzymes can be swallowed whole or sprinkled on a small amount of food taken at the beginning of a meal. This choice is a valid option for administering pancreatic enzymes. While it's true that the enzymes can be taken either by swallowing the capsules whole or by opening them and sprinkling the contents on a small amount of food at the start of a meal, this method can vary based on individual preferences and abilities. However, the primary focus should be on timing (between meals) to achieve the best enzymatic action.
Choice C rationale:
Do not administer pancreatic enzymes if the child is receiving antibiotics. This statement is not accurate. There is no general contraindication to administering pancreatic enzymes while a child is on antibiotics. However, it's important for the healthcare provider to be aware of all the medications the child is taking to ensure there are no potential drug interactions or effects on absorption. Always consult with the healthcare team before adjusting the administration of any medication.
Choice D rationale:
Decrease the dose of pancreatic enzymes if the child is having frequent, bulky stools. This statement is not consistent with typical practice. If a child is experiencing frequent, bulky stools, it may actually indicate that the pancreatic enzyme dosage needs adjustment (increasing the dose rather than decreasing). Bulky stools can suggest poor digestion and absorption, which might require more enzymes to properly break down nutrients. Dosage adjustments should always be made under the guidance of the healthcare provider based on factors such as stool consistency, weight gain, and nutritional status.